

Dynamics of human regulatory T cells in lung lavages of lung transplant recipients
- PMID: 19696635
- PMCID: PMC2773802
- DOI: 10.1097/TP.0b013e3181b0e719
Dynamics of human regulatory T cells in lung lavages of lung transplant recipients
Abstract
Background: Despite advances in the field of lung transplantation, the median survival after lung transplant remains below 5 years. Early rejection is a risk factor for the development of chronic rejection. In animal models of transplant tolerance, regulatory T cells (Tregs) can prevent the establishment of rejection.
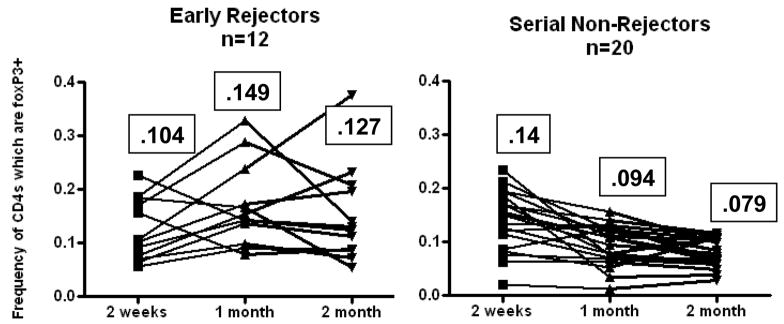
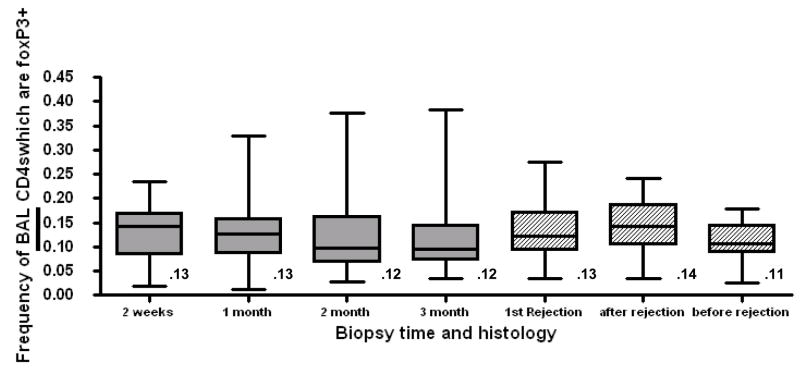
Methods: This study was designed to explore the dynamics of Tregs focally and systemically in lung transplant recipients. Sequential surveillance bronchoscopy results were available in 51 patients with at least four sequential samples recovered from each patient at defined times posttransplant. In 36 individuals, a complete year of follow-up data for BAL was analyzed. In 33 of these individuals had a complete year of follow-up data for peripheral blood monocyte cell specimens were also analyzed. Lung lavage cells were recovered from each bronchoscopy and corresponding blood draw and subjected to polychromatic flow cytometry. The percentage of CD4 lymphocytes, which expressed the intracellular transcription factor FoxP3 was recorded at each point. At each time point, lung biopsy specimens were scored for rejection.
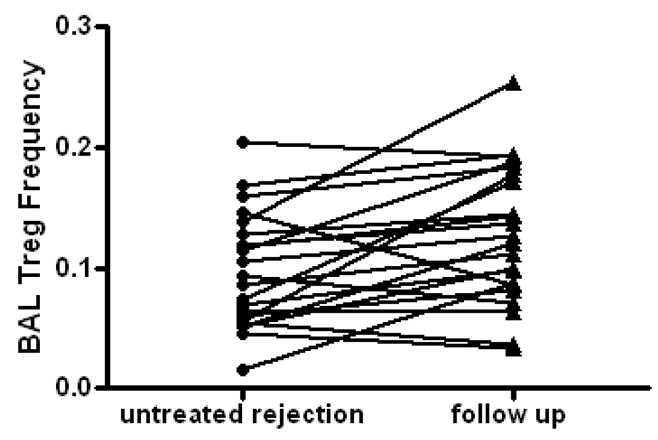
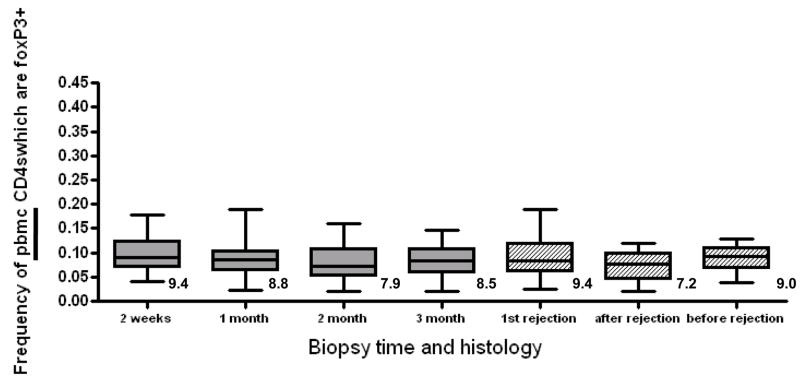
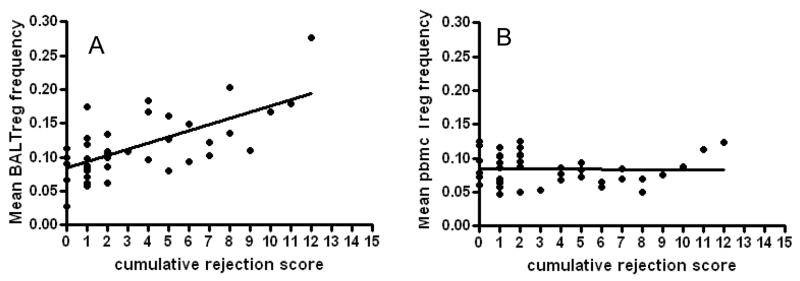
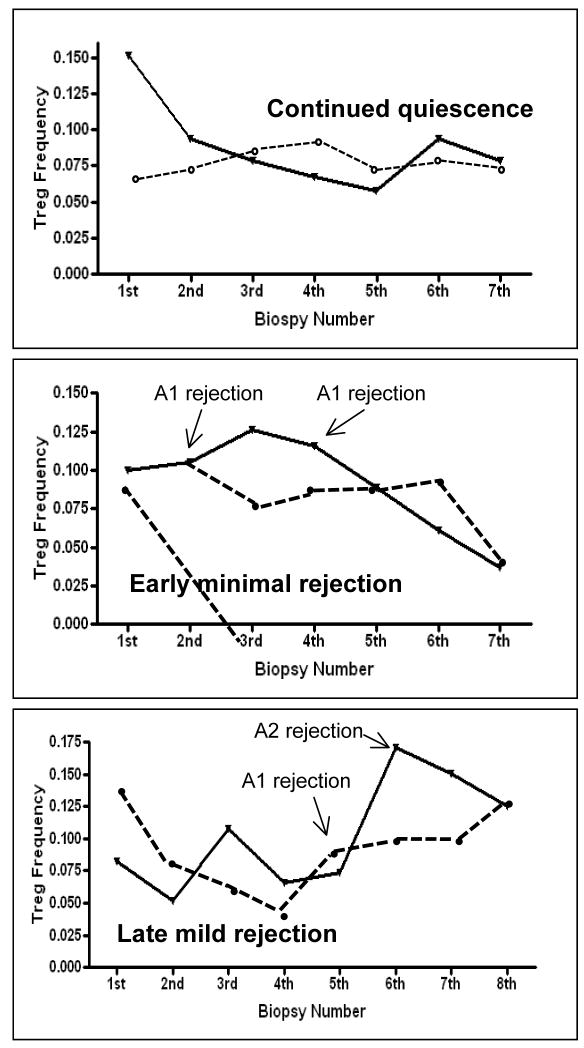
Results: Lung Treg frequency was significantly more variable than blood Treg frequency. Treg frequency in the lung was increased in the aftermath of acute rejection. In contrast, lung Treg frequency declined sequentially in patients demonstrating continued quiescence. Mean BAL Treg level integrated over the first transplant year correlated inversely with the degree of acute cellular rejection. In contrast, blood Treg levels demonstrated no correlation with lung pathology.
Conclusions: Lung Tregs increase in the setting of acute cellular rejection, whereas declining levels of BAL Tregs correlates with immunologic quiescence.
Figures
References
-
- Hertz MI, Aurora P, Boucek MM, et al. Registry of the International Society for Heart and Lung Transplantation: introduction to the 2007 annual reports--100,000 transplants and going strong. J Heart Lung Transplant. 2007;26 (8):763. - PubMed
-
- Lau CL, Palmer SM, Posther KE, et al. Influence of panel-reactive antibodies on posttransplant outcomes in lung transplant recipients. Ann Thorac Surg. 2000;69 (5):1520. - PubMed
-
- Khalifah AP, Hachem RR, Chakinala MM, et al. Respiratory viral infections are a distinct risk for bronchiolitis obliterans syndrome and death. Am J Respir Crit Care Med. 2004;170 (2):181. - PubMed
-
- Billings JL, Hertz MI, Savik K, Wendt CH. Respiratory viruses and chronic rejection in lung transplant recipients. J Heart Lung Transplant. 2002;21 (5):559. - PubMed
-
- D’Ovidio F, Mura M, Tsang M, et al. Bile acid aspiration and the development of bronchiolitis obliterans after lung transplantation. J Thorac Cardiovasc Surg. 2005;129 (5):1144. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
