

Relation of left ventricular mass and concentric remodeling to extent of coronary artery disease by computed tomography in patients without left ventricular hypertrophy: ROMICAT study
- PMID: 19696685
- PMCID: PMC2875785
- DOI: 10.1097/HJH.0b013e328331054a
Relation of left ventricular mass and concentric remodeling to extent of coronary artery disease by computed tomography in patients without left ventricular hypertrophy: ROMICAT study
Abstract
Objective: Cardiac computed tomography allows for simultaneous assessment of left ventricular mass (LVM) and coronary artery disease (CAD). We aimed to determine whether LVM, LVM index (LVMi), and the left ventricular geometric pattern of concentric remodeling are associated with the extent of CAD in patients without left ventricular hypertrophy.
Methods: In 348 patients from the Rule Out Myocardial Infarction Using Computer Assisted Tomography trial, 64-slice computed tomography was performed and LVM measured at end-diastole. We used three LVM indexation criteria to obtain three cohorts: LVM indexed to body surface area by echocardiography (n = 337) and computed tomography criteria (n = 325), and by height (n = 326). The cohorts were subdivided into concentric remodeling and normal geometry. Extent of coronary plaque was classified based on a 17-segment model, treated as a continuous variable, and stratified into three groups: zero segment, one to four segments, and more than four segments.
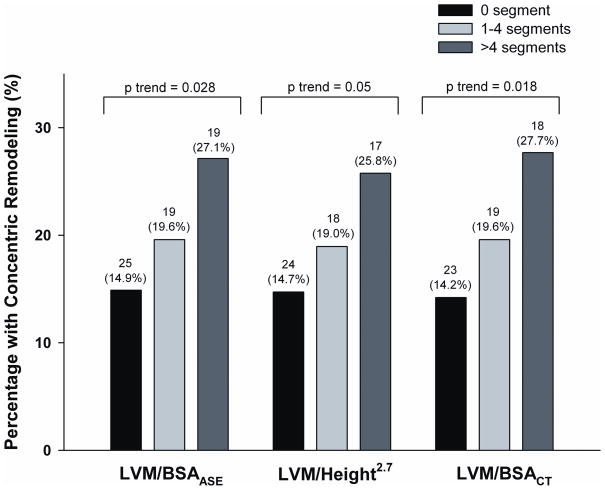
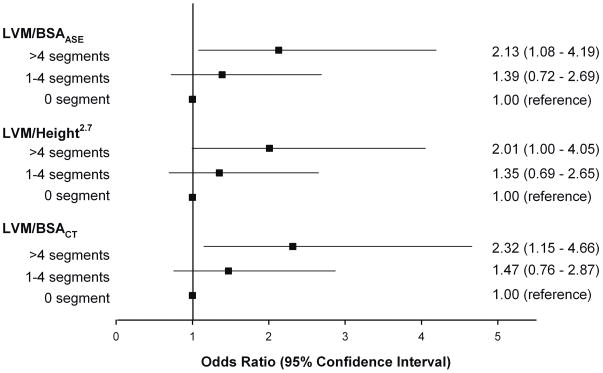
Results: Patients with more than four segments of coronary plaque had higher LVM (Delta12.8-15.1 g) and LVMi (Delta4.0-5.5 g/m and Delta2.2 g/m) than those without CAD (all P < or = 0.03). After multivariable adjustment, LVM and LVMi remained independent predictors of extent of coronary plaque, with 0.27-0.29 segments more plaque per 20 g increase of LVM (all P = 0.02), 0.32-0.34 segments more plaque per 10 g/m increase of LVMi (both P = 0.02), and 0.80 segments more plaque per 10 g/m increase of LVMi (P = 0.008). Concentric remodeling patients had 1.1-1.3 segments more plaque than those with normal geometry (all P < or = 0.05). Patients with more than four segments of plaque had two-fold increase in odds (all P < or = 0.05) of having concentric remodeling as compared with those without CAD.
Conclusion: Increased LVM, LVMi, and concentric remodeling are associated with a greater degree of coronary plaque burden in patients without left ventricular hypertrophy. These findings could provide an indication to intensify medical therapy in patients with subclinical CAD and hypertension.
Conflict of interest statement
Figures
References
-
- Verma A, Meris A, Hicham S, Ghali JK, Arnold JMO, Bourgoun M, et al. Prognostic Implications of Left Ventricular Mass and Geometry Following Myocardial Infarction. J Am Coll Cardiol Img. 2008;1:582–591. - PubMed
-
- Gottdiener JS, Arnold AM, Aurigemma GP, Polak JF, Tracy RP, Kitzman DW, et al. Predictors of congestive heart failure in the elderly: the Cardiovascular Health Study. J Am Coll Cardiol. 2000;35:1628–1637. - PubMed
-
- Drazner MH, Rame JE, Marino EK, Gottdiener JS, Kitzman DW, Gardin JM, et al. Increased left ventricular mass is a risk factor for the development of a depressed left ventricular ejection fraction within five years: the Cardiovascular Health Study. J Am Coll Cardiol. 2004;43:2207–2215. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
