

White blood cell count predicts all-cause mortality in patients with suspected peripheral arterial disease
- PMID: 19699384
- PMCID: PMC2785081
- DOI: 10.1016/j.amjmed.2009.02.020
White blood cell count predicts all-cause mortality in patients with suspected peripheral arterial disease
Abstract
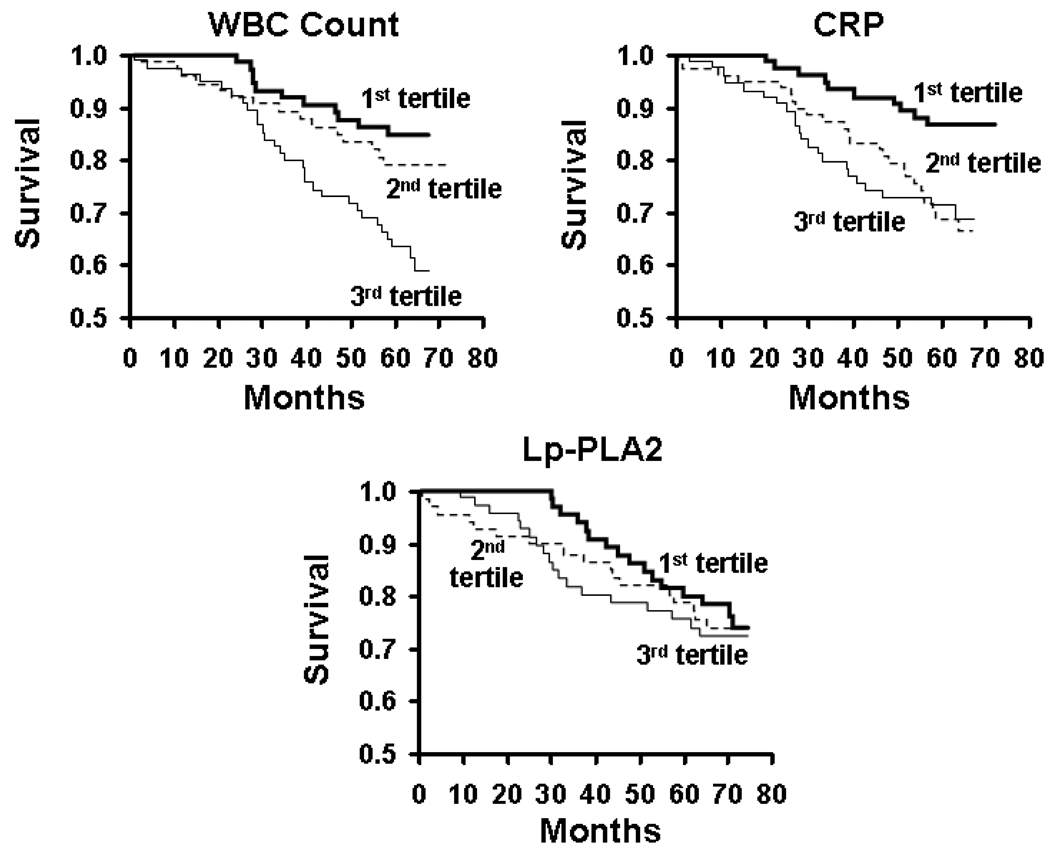
Objective: We investigated whether markers of inflammation-white blood cell (WBC) count, C-reactive protein (CRP), and lipoprotein-associated phospholipase A2-are associated with mortality in patients referred for noninvasive lower-extremity arterial evaluation.
Methods: Participants (n = 242, mean age 68 years, 54% men) were followed for a median of 71 months. Ankle-brachial index (ABI), WBC count, plasma CRP, and lipoprotein-associated phospholipase A2 were measured at the start of the study. Factors associated with all-cause mortality were identified using Cox proportional hazards.
Results: During the follow-up period, 56 patients (25%) died. Factors associated with higher mortality were greater age, history of coronary artery disease/cerebrovascular disease, lower ABI, higher serum creatinine, and higher WBC count/plasma CRP. In stepwise multivariable regression analysis, ABI, serum creatinine, WBC count, and CRP were associated significantly with mortality. Patients in the top tertile of WBC count and CRP level had a relative risk of mortality of 3.37 (confidence interval [CI], 1.56-7.27) and 2.12 (CI, 0.97-4.62), respectively. However, only the WBC count contributed incrementally to prediction of mortality. Inferences were similar when analyses were limited to patients with peripheral arterial disease (ABI<0.9, n = 114).
Conclusion: WBC count, but not plasma CRP level, provides incremental information about the risk of death in patients referred for lower-extremity arterial evaluation and in the subset of these patients with peripheral arterial disease.
Figures
References
-
- Rosamond W, Flegal K, Friday G, Furie K, Go A, Greenlund K, Haase N, Ho M, Howard V, Kissela B, Kittner S, Lloyd-Jones D, McDermott M, Meigs J, Moy C, Nichol G, O'Donnell CJ, Roger V, Rumsfeld J, Sorlie P, Steinberger J, Thom T, Wasserthiel-Smoller S, Hong Y. Heart disease and stroke statistics--2007 update: a report from the American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Circulation. 2007;115(5):e69–e171. - PubMed
-
- Criqui MH, Langer RD, Fronek A, Feigelson HS, Klauber MR, McCann TJ, Browner D. Mortality over a period of 10 years in patients with peripheral arterial disease. New England Journal of Medicine. 1992;326(6):381–386. - PubMed
-
- Steg PG, Bhatt DL, Wilson PWF, D'Agostino R, Sr, Ohman EM, Rother J, Liau C-S, Hirsch AT, Mas J-L, Ikeda Y, Pencina MJ, Goto S, Investigators RR. One-year cardiovascular event rates in outpatients with atherothrombosis.[see comment] JAMA. 2007;297(11):1197–1206. - PubMed
-
- Grundy SM, Cleeman JI, Merz CNB, Brewer HB, Jr, Clark LT, Hunninghake DB, Pasternak RC, Smith SC, Jr, Stone NJ National Heart LaBI, American College of Cardiology F, American Heart A. Implications of recent clinical trials for the National Cholesterol Education Program Adult Treatment Panel III guidelines.[erratum appears in Circulation. 2004 Aug 10;110(6):763] Circulation. 2004;110(2):227–239. - PubMed
-
- Libby P. Inflammation in atherosclerosis. Nature. 2002;420(6917):868–874. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
