

Amniotic membrane transplantation as a new therapy for the acute ocular manifestations of Stevens-Johnson syndrome and toxic epidermal necrolysis
- PMID: 19699503
- PMCID: PMC2853888
- DOI: 10.1016/j.survophthal.2009.03.004
Amniotic membrane transplantation as a new therapy for the acute ocular manifestations of Stevens-Johnson syndrome and toxic epidermal necrolysis
Abstract
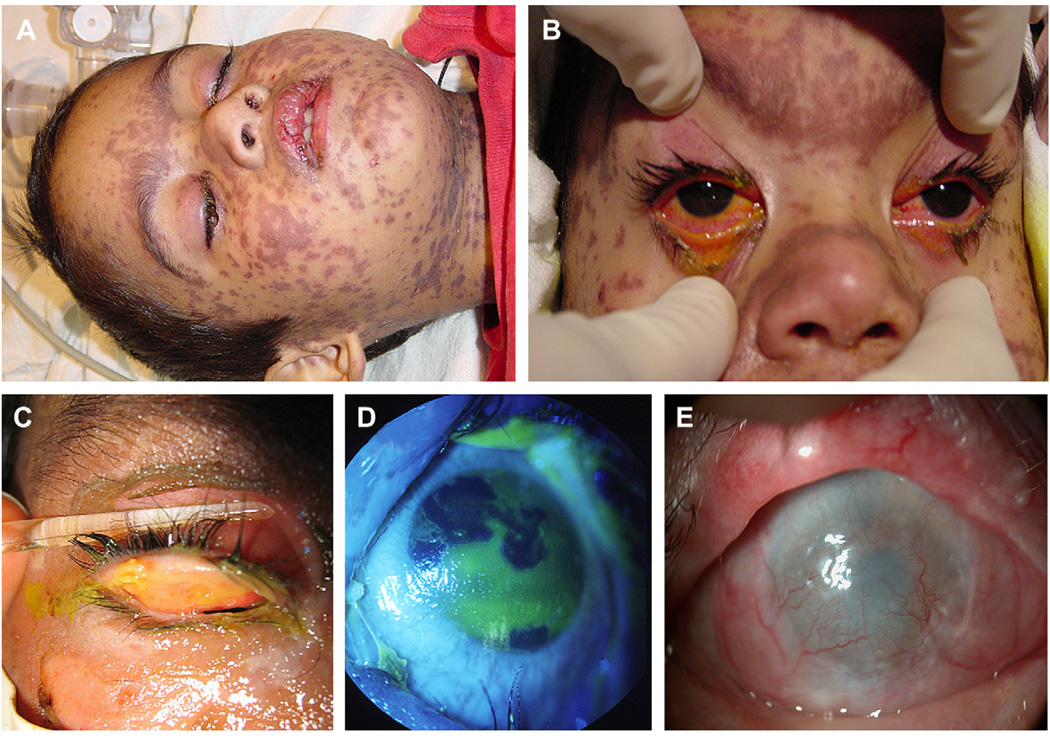
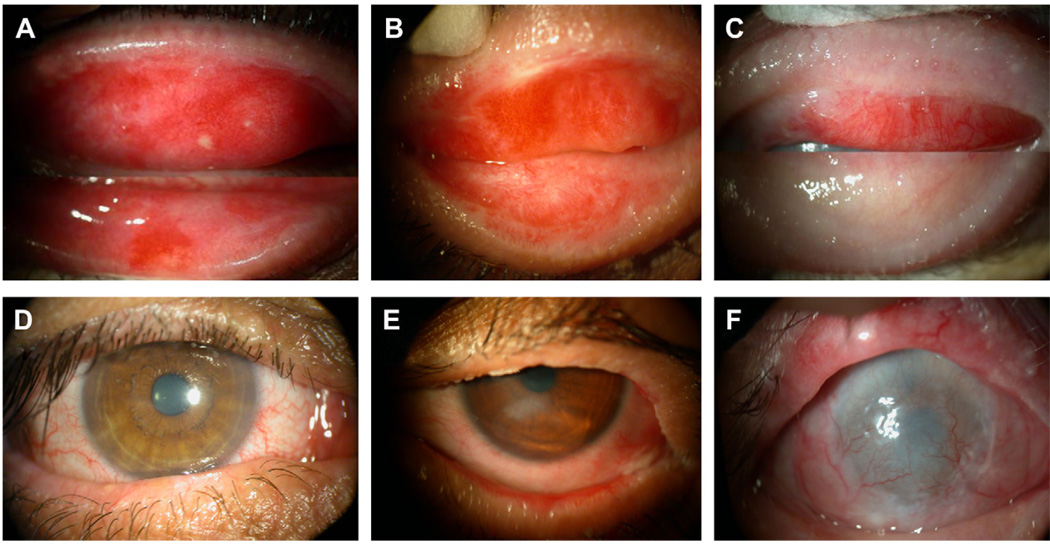
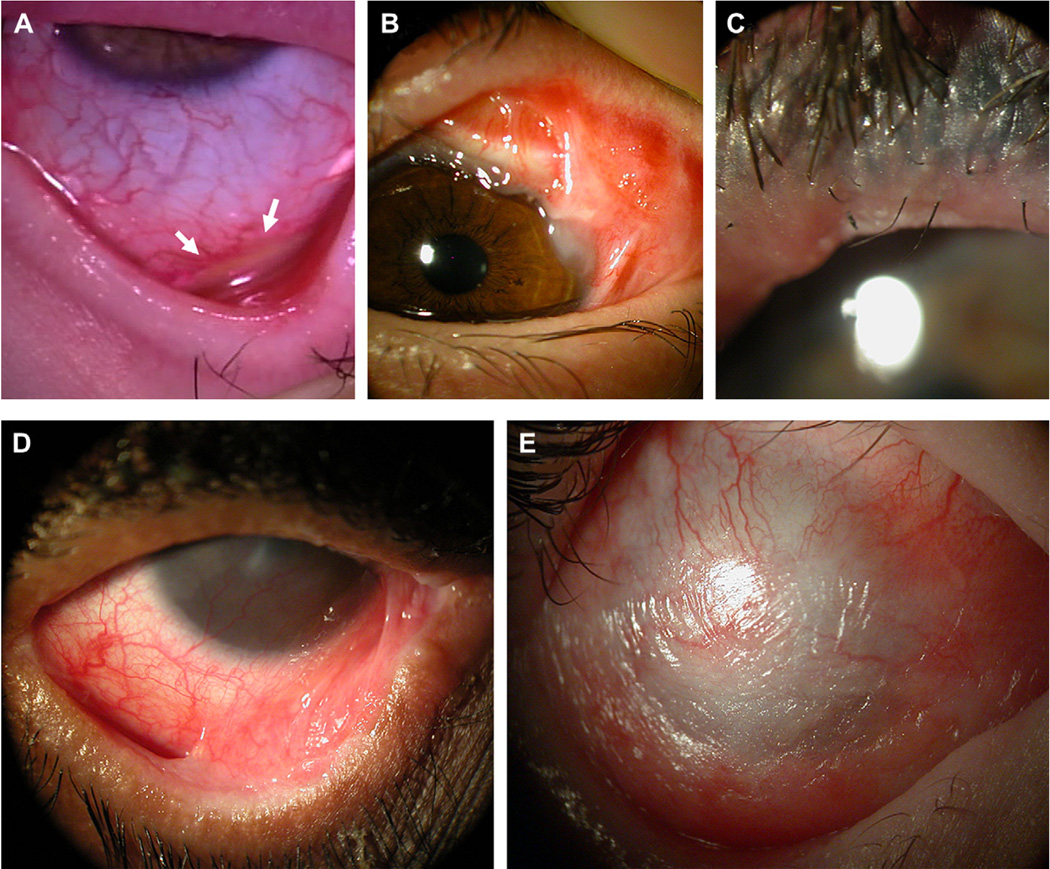
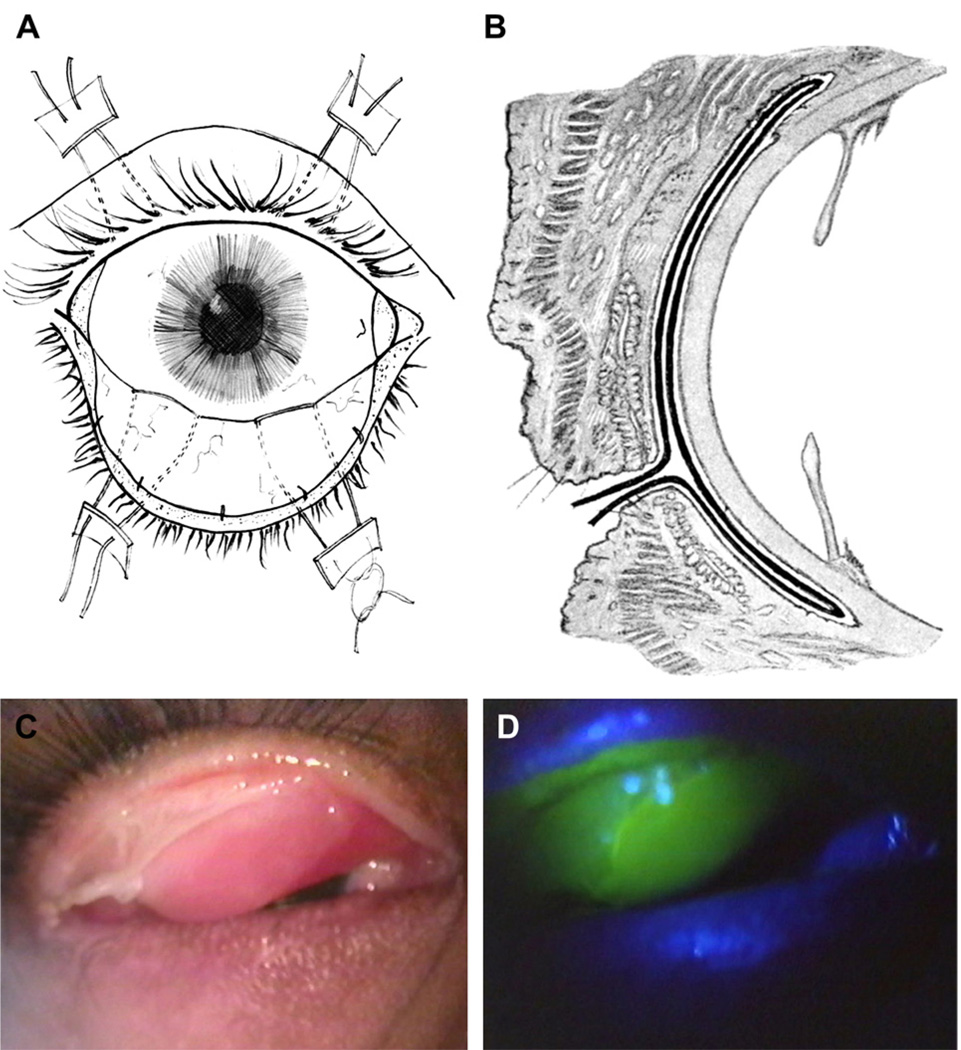
Stevens-Johnson syndrome and its more severe variant, toxic epidermal necrolysis, have relatively low overall incidence; however, this disease presents with high morbidity and mortality. The majority of patients develop ocular inflammation and ulceration at the acute stage. Due to the hidden nature of these ocular lesions and the concentration of effort toward life-threatening issues, current acute management has not devised a strategy to preclude blinding cicatricial complications. This review summarizes recent literature data, showing how sight-threatening corneal complications can progressively develop from cicatricial pathologies of lid margin, tarsus, and fornix at the chronic stage. It illustrates how such pathologies can be prevented with the early intervention of cryopreserved amniotic membrane transplantation to suppress inflammation and promote epithelial healing at the acute stage. Significant dry eye problems and photophobia can also be avoided with this intervention. This new therapeutic strategy can avert the catastrophic ophthalmic sequelae of this rare but devastating disease.
Figures
References
-
- Aihara Y, Ito R, Ito S, et al. Toxic epidermal necrolysis in a child successfully treated with cyclosporin A and methyl-prednisolone. Pediatr Int. 2007 Oct;49(5):659–662. - PubMed
-
- Arevalo JM, Lorente JA, Gonzalez-Herrada C, Jimenez-Reyes J. Treatment of toxic epidermal necrolysis with cyclosporin A. J Trauma. 2000;48(3):473–478. - PubMed
-
- Arora R, Mehta D, Jain V. Amniotic membrane transplantation in acute chemical burns. Eye. 2005 Mar;19(3):273–278. - PubMed
-
- Arstikaitis MJ. Ocular aftermath of Stevens-Johnson syndrome. Arch Ophthalmol. 1973 Nov;90(5):376–379. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
