

Clinical and microbiological benefits of strict supragingival plaque control as part of the active phase of periodontal therapy
- PMID: 19703236
- PMCID: PMC2744842
- DOI: 10.1111/j.1600-051X.2009.01471.x
Clinical and microbiological benefits of strict supragingival plaque control as part of the active phase of periodontal therapy
Abstract
Aim: To compare the clinical and microbiological effects of scaling and root planing (SRP) alone or combined with mechanical [professional plaque control (PPC)] or chemical [chlorhexidine rinsing (CHX)] control of supragingival plaque in the treatment of chronic periodontitis.
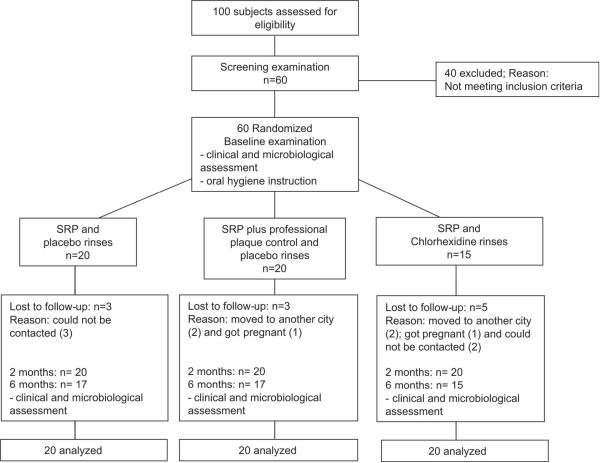
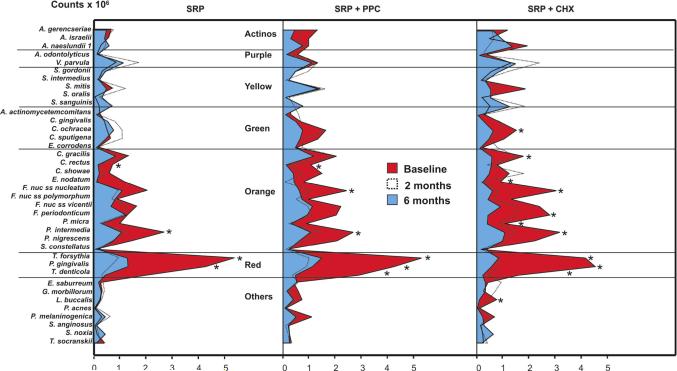
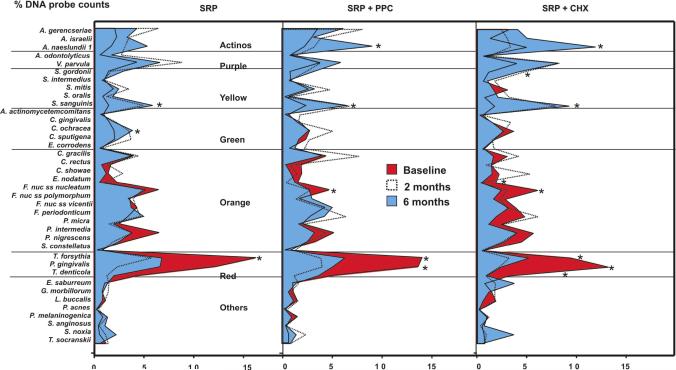
Material and methods: Sixty subjects were randomly assigned to receive SRP alone or combined with PPC (twice a week) or with CHX rinsing (twice a day). The adjunctive treatments began with SRP and were continued for 42 days. Clinical and microbiological examinations were performed at baseline, 2 and 6 months post-therapy. Subgingival plaque samples were analysed for 38 bacterial species by checkerboard DNA-DNA hybridization.
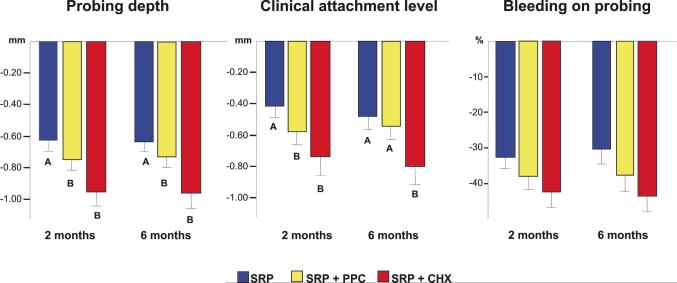
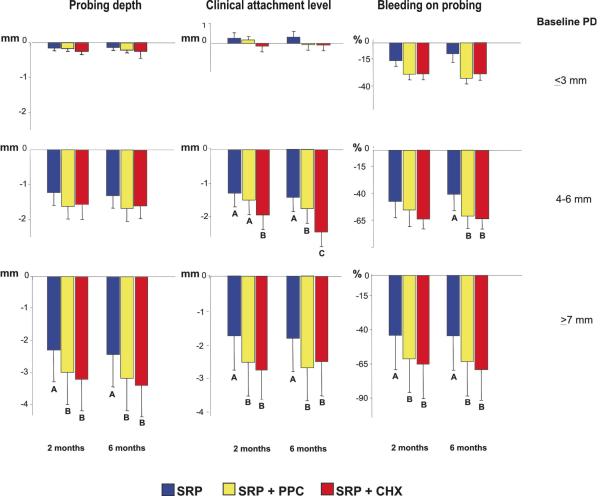
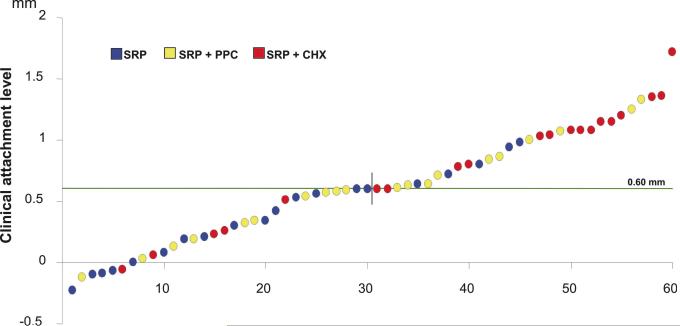
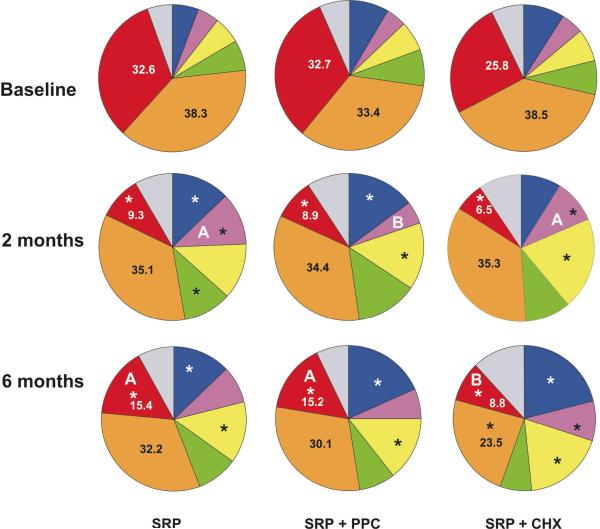
Results: The two test treatments were more effective in improving probing depth and clinical attachment level (CAL) than SRP alone, even in intermediate and deep sites. CAL gain was better maintained in the CHX group. The most beneficial microbiological changes were observed in CHX-treated subjects, who showed a significant reduction in the proportions of red and orange complexes, as well as an increase in the proportions of the host-compatible bacterial species.
Conclusion: Strict plaque control performed during and after SRP improves periodontal treatment outcomes. The greatest microbiological and clinical benefits were observed with the use of CHX rinsing.
Figures
References
-
- Araújo MW, Hovey KM, Benedek JR, Grossi SG, Dorn J, Wactawski-Wnde J, Genco RJ, Trevisan M. Reproducibility of probing depth measurement using a constant-force electronic probe: analysis of inter and intraexaminer variability. Journal of Periodontoly. 2003;74:1736–1740. - PubMed
-
- Armitage GC. Development of a classification system for periodontal diseases and conditions. Annals of Periodontology. 1999;4:1–6. - PubMed
-
- Carvalho LH, D'Avila GB, Leão A, Haffajee AD, Socransky SS, Feres M. Scaling and root planing, systemic metronidazole and Professional plaque removal in the treatment of chronic periodontitis in a Brazilian population. Journal of Clinical Periodontology. 2004;31:1070–1076. - PubMed
-
- Carvalho LH, D'Avila GB, Leão A, Gonçalves C, Haffajee AD, Socransky SS, Feres M. Scaling and root planning, systemic metronidazole and professional plaque removal in the treatment of chronic periodontitis in a Brazilian population II - microbiological results. Journal of Clinical Periodontology. 2005;32:406–411. - PubMed
-
- De Soete M, Mongardini C, Peuwels M, Haffajee AD, Socransky SS, van Steenberghe D, Quirynen M. One-stage full-mouth disinfection. Long-term microbiological results analyzed by checkerboard DNA-DNA hybridization. Journal of Periodontology. 2001;72:374–382. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
