

Muscle sympathetic nerve activity during intense lower body negative pressure to presyncope in humans
- PMID: 19703962
- PMCID: PMC2770161
- DOI: 10.1113/jphysiol.2009.177352
Muscle sympathetic nerve activity during intense lower body negative pressure to presyncope in humans
Abstract
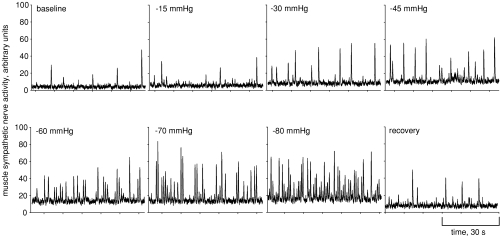
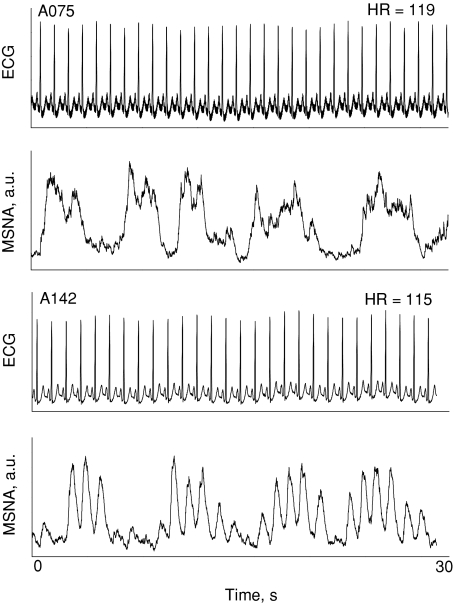
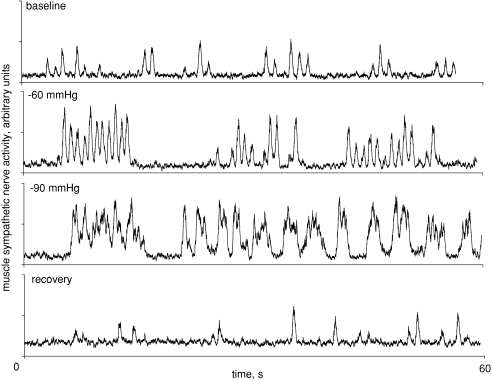
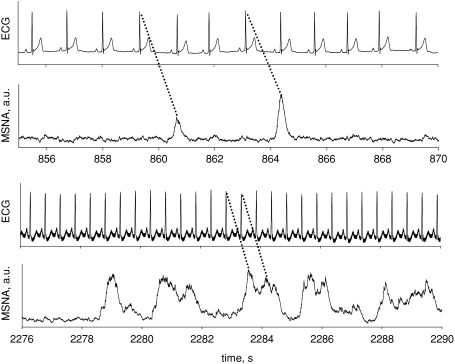
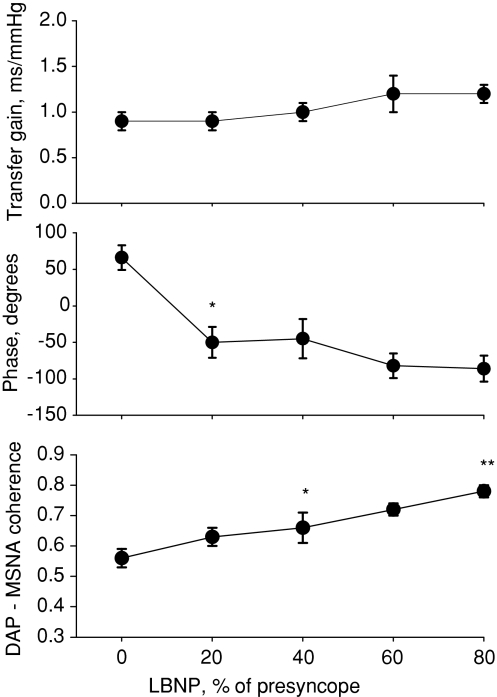
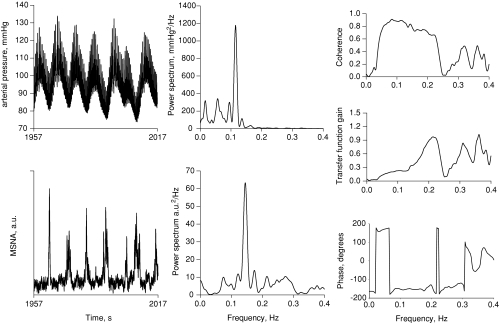
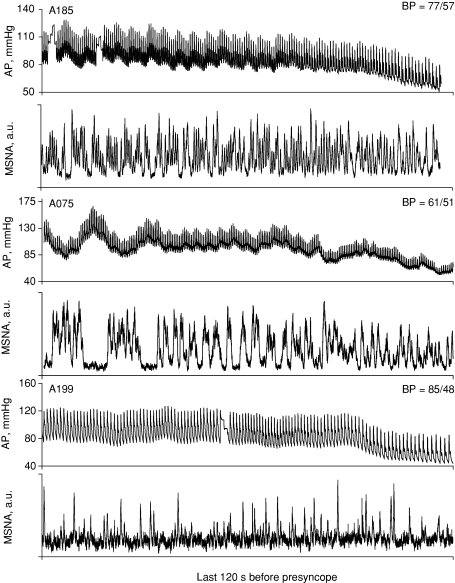
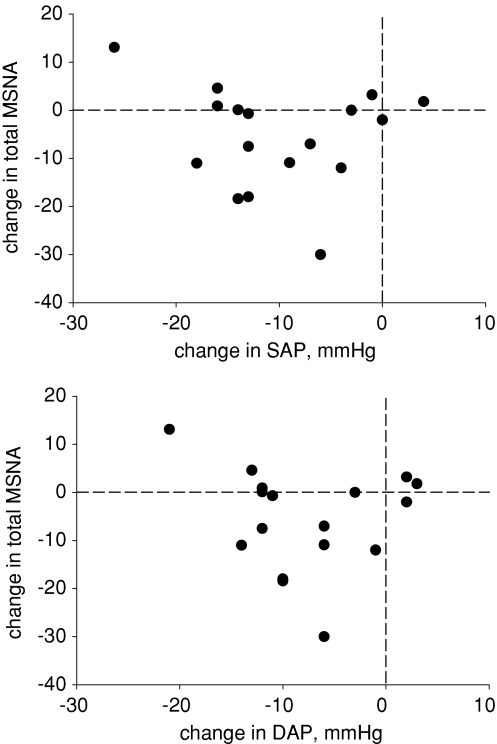
Activation of sympathetic efferent traffic is essential to maintaining adequate arterial pressures during reductions of central blood volume. Sympathetic baroreflex gain may be reduced, and muscle sympathetic firing characteristics altered with head-up tilt just before presyncope in humans. Volume redistributions with lower body negative pressure (LBNP) are similar to those that occur during haemorrhage, but limited data exist describing arterial pressure-muscle sympathetic nerve activity (MSNA) relationships during intense LBNP. Responses similar to those that occur in presyncopal subjects during head-up tilt may signal the beginnings of cardiovascular decompensation associated with haemorrhage. We therefore tested the hypotheses that intense LBNP disrupts MSNA firing characteristics and leads to a dissociation between arterial pressure and sympathetic traffic prior to presyncope. In 17 healthy volunteers (12 males and 5 females), we recorded ECG, finger photoplethysmographic arterial pressure and MSNA. Subjects were exposed to 5 min LBNP stages until the onset of presyncope. The LBNP level eliciting presyncope was denoted as 100% tolerance, and then data were assessed relative to this normalised maximal tolerance by expressing LBNP levels as 80, 60, 40, 20 and 0% (baseline) of maximal tolerance. Data were analysed in both time and frequency domains, and cross-spectral analyses were performed to determine the coherence, transfer function and phase angle between diastolic arterial pressure (DAP) and MSNA. DAP-MSNA coherence increased progressively and significantly up to 80% maximal tolerance. Transfer functions were unchanged, but phase angle shifted from positive to negative with application of LBNP. Sympathetic bursts fused in 10 subjects during high levels of LBNP (burst fusing may reflect modulation of central mechanisms, an artefact arising from our use of a 0.1 s time constant for integrating filtered nerve activity, or a combination of both). On average, arterial pressures and MSNA decreased significantly the final 20 s before presyncope (n = 17), but of this group, MSNA increased in seven subjects. No linear relationship was observed between the magnitude of DAP and MSNA changes before presyncope (r = 0.12). We report three primary findings: (1) progressive LBNP (and presumed progressive arterial baroreceptor unloading) increases cross-spectral coherence between arterial pressure and MSNA, but sympathetic baroreflex control is reduced before presyncope; (2) withdrawal of MSNA is not a prerequisite for presyncope despite significant decreases of arterial pressure; and (3) reductions of venous return, probably induced by intense LBNP, disrupt MSNA firing characteristics that manifest as fused integrated bursts before the onset of presyncope. Although fusing of integrated sympathetic bursts may reflect a true physiological compensation to severe reductions of venous return, duplication of this finding utilizing shorter time constants for integration of the nerve signal is required.
Figures
Comment in
-
Orthostatic stress, haemorrhage and a bankrupt cardiovascular system.J Physiol. 2009 Nov 1;587(Pt 21):5015-6. doi: 10.1113/jphysiol.2009.181495. Epub 2009 Sep 21. J Physiol. 2009. PMID: 19770188 Free PMC article. No abstract available.
-
Role of SNA in the pathophysiology of cardiovascular collapse during syncope: muscle vs. brain.J Physiol. 2009 Dec 1;587(Pt 23):5795-6. doi: 10.1113/jphysiol.2009.182667. J Physiol. 2009. PMID: 19959554 Free PMC article. No abstract available.
References
-
- Barman SM, Fadel PJ, Vongpatanasin W, Victor RG, Gebber GL. Basis for the cardiac-related rhythm in muscle sympathetic nerve activity of humans. Am J Physiol Heart Circ Physiol. 2003;284:H584–H597. - PubMed
-
- Batchinsky AI, Cooke WH, Kuusela TA, Jordan BS, Wang JJ, Cancio LC. Sympathetic nerve activity and heart rate variability during severe hemorrhagic shock in sheep. Auton Neurosci. 2007;136:43–51. - PubMed
-
- Convertino VA, Ludwig DA, Cooke WH. Stroke volume and sympathetic responses to lower-body negative pressure reveal new insight into circulatory shock in humans. Auton Neurosci. 2004;111:127–134. - PubMed
-
- Cooke WH, Convertino VA. Association between vasovagal hypotension and low sympathetic neural activity during presyncope. Clin Auton Res. 2002;12:483–486. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical