

Maximizing survival benefit with primary prevention implantable cardioverter-defibrillator therapy in a heart failure population
- PMID: 19704100
- PMCID: PMC3774781
- DOI: 10.1161/CIRCULATIONAHA.108.816884
Maximizing survival benefit with primary prevention implantable cardioverter-defibrillator therapy in a heart failure population
Abstract
Background: Although implantable cardioverter-defibrillator (ICD) therapy reduces mortality in moderately symptomatic heart failure patients with an ejection fraction <or=35%, many such patients do not require ICD shocks over long-term follow-up.
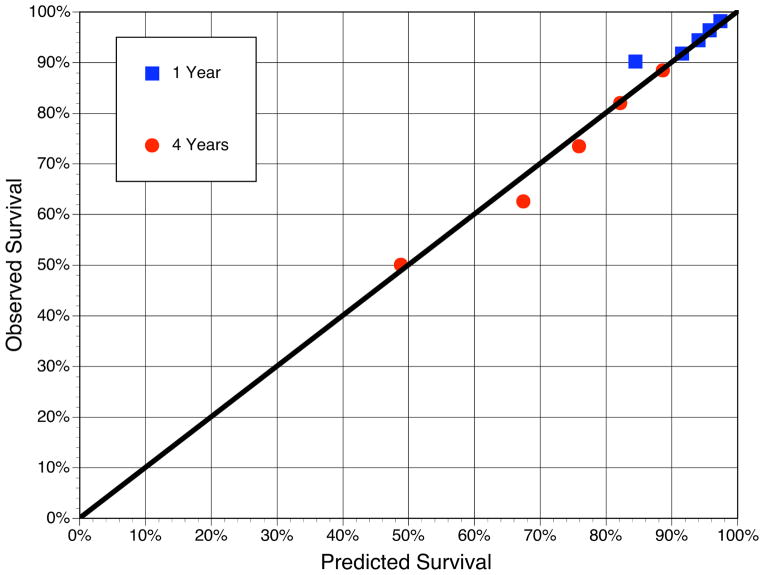
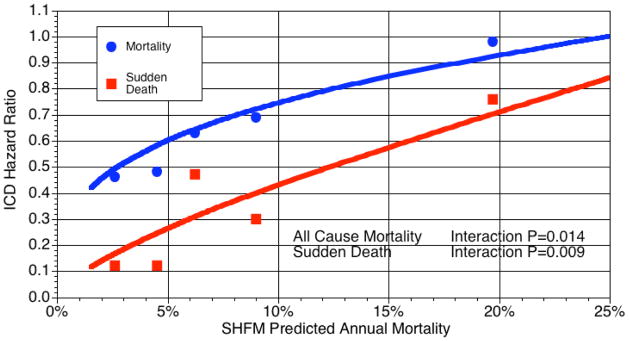
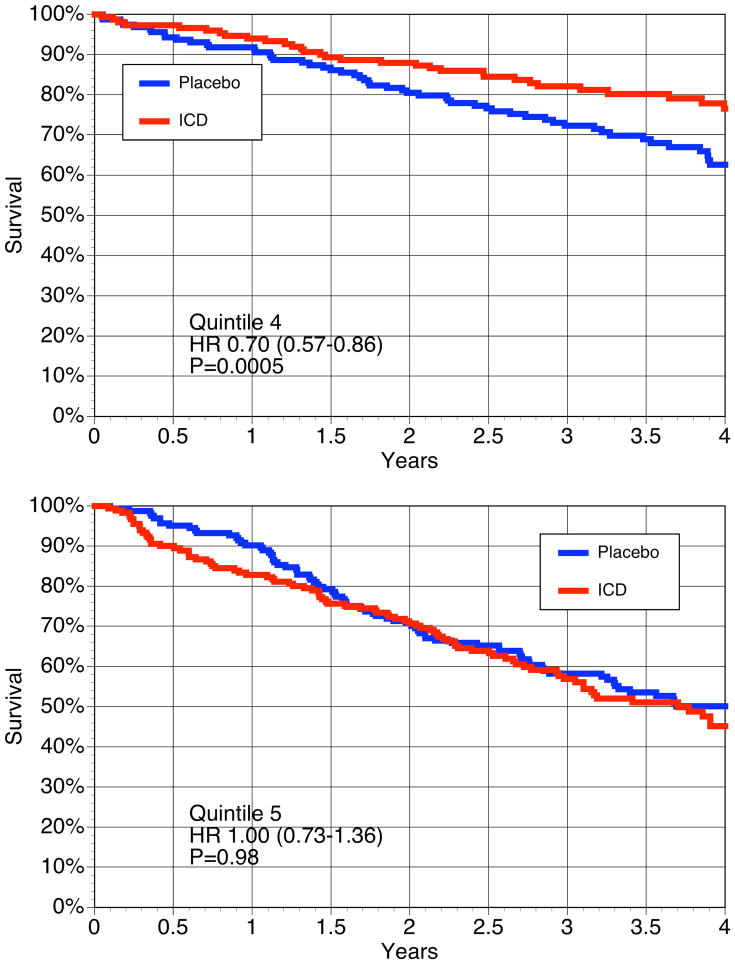
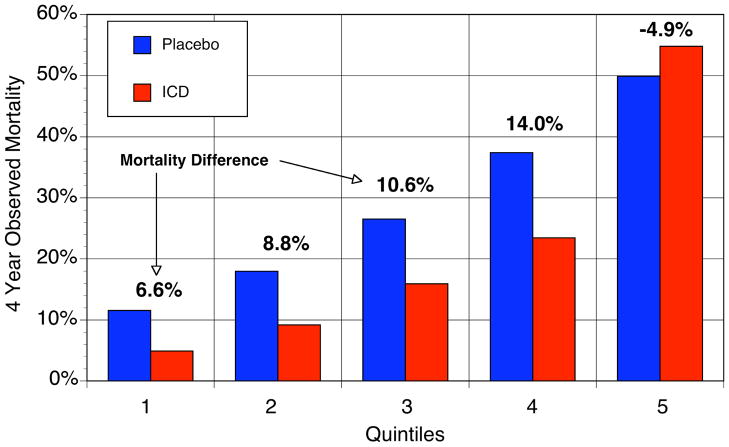
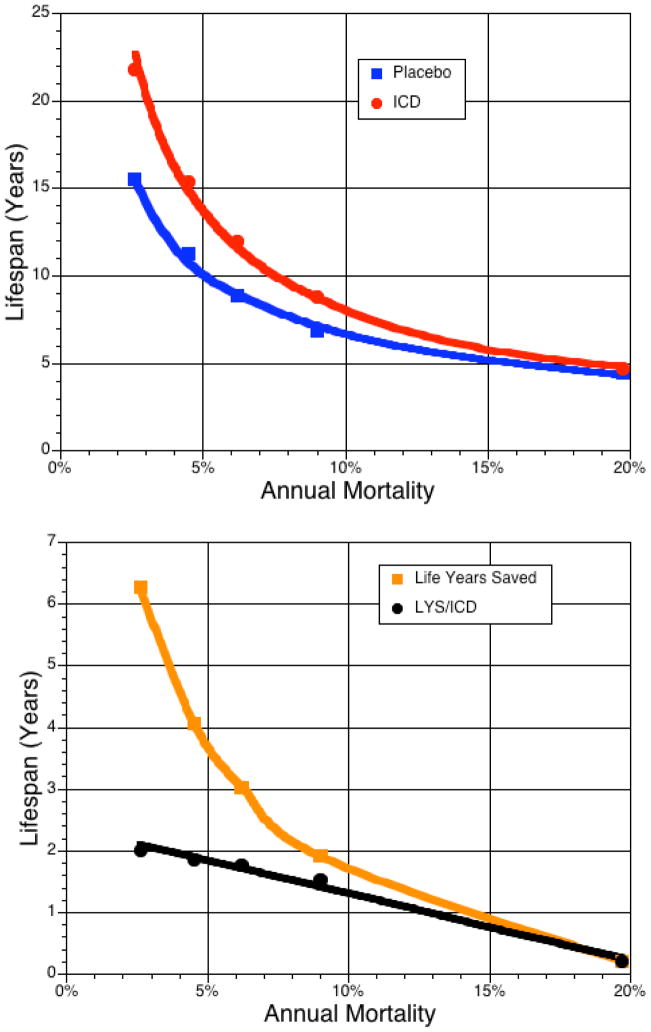
Methods and results: Using a modification of a previously validated risk prediction model based on routine clinical variables, we examined the relationship between baseline predicted mortality risk and the relative and absolute survival benefits of ICD treatment in the primary prevention Sudden Cardiac Death in Heart Failure Trial (SCD-HeFT). In the placebo arm, predicted 4-year mortality grouped into 5 equal-sized risk groups varied from 12% to 50% (c statistic=0.71), whereas the proportion of SCD in those same risk groups decreased from 52% to 24% of all deaths. ICD treatment decreased relative risk of SCD by 88% in the lowest-risk group versus 24% in the highest-risk group (P=0.009 for interaction) and decreased relative risk of total mortality by 54% in the lowest-risk group versus no benefit (2%) in the highest-risk group (P=0.014 for interaction). Absolute 4-year mortality reductions were 6.6%, 8.8%, 10.6%, 14.0%, and -4.9% across risk quintiles. In highest-risk patients (predicted annual mortality >20%), no benefit of ICD treatment was seen. Projected over each patient's predicted lifespan, ICD treatment added 6.3, 4.1, 3.0, 1.9, and 0.2 additional years of life in the lowest- to highest-risk groups, respectively.
Conclusions: A clinical risk prediction model identified subsets of moderately symptomatic heart failure patients in SCD-HeFT in whom single-lead ICD therapy was of no benefit and other subsets in which benefit was substantial.
Trial registration: ClinicalTrials.gov NCT00000609.
Figures


Comment in
-
Refining patient selection for primary prevention implantable cardioverter-defibrillator therapy: reeling in a net cast too widely.Circulation. 2009 Sep 8;120(10):825-7. doi: 10.1161/CIRCULATIONAHA.109.891069. Epub 2009 Aug 24. Circulation. 2009. PMID: 19704090 No abstract available.
References
-
- Hunt SA, Abraham WT, Chin MH, Feldman AM, Francis GS, Ganiats TG, Jessup M, Konstam MA, Mancini DM, Michl K, Oates JA, Rahko PS, Silver MA, Stevenson LW, Yancy CW, Antman EM, Smith SC, Jr, Adams CD, Anderson JL, Faxon DP, Fuster V, Halperin JL, Hiratzka LF, Jacobs AK, Nishimura R, Ornato JP, Page RL, Riegel B. ACC/AHA 2005 Guideline Update for the Diagnosis and Management of Chronic Heart Failure in the Adult. Circulation. 2005;112:e154–235. - PubMed
-
- Epstein AE, Dimarco JP, Ellenbogen KA, Estes NA, 3rd, Freedman RA, Gettes LS, Gillinov AM, Gregoratos G, Hammill SC, Hayes DL, Hlatky MA, Newby LK, Page RL, Schoenfeld MH, Silka MJ, Stevenson LW, Sweeney MO. ACC/AHA/HRS 2008 Guidelines for Device-Based Therapy of Cardiac Rhythm Abnormalities. Circulation. 2008;117:e350–408. - PubMed
-
- Feder B. New York Times. New York: 2008. Defibrillators are lifesaver, but risk gives pause (September 13, 2008) p. 1.
-
- Buxton AE, Lee KL, Hafley GE, Pires LA, Fisher JD, Gold MR, Josephson ME, Lehmann MH, Prystowsky EN. Limitations of ejection fraction for prediction of sudden death risk in patients with coronary artery disease: lessons from the MUSTT study. J Am Coll Cardiol. 2007;50:1150–7. - PubMed
-
- Bardy GH, Lee KL, Mark DB, Poole JE, Packer DL, Boineau R, Domanski M, Troutman C, Anderson J, Johnson G, McNulty SE, Clapp-Channing N, Davidson-Ray LD, Fraulo ES, Fishbein DP, Luceri RM, Ip JH. Amiodarone or an implantable cardioverter-defibrillator for congestive heart failure. N Engl J Med. 2005;352:225–37. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
