

Therapeutic options in the management of acromegaly: focus on lanreotide Autogel
- PMID: 19707377
- PMCID: PMC2721386
- DOI: 10.2147/btt.s3356
Therapeutic options in the management of acromegaly: focus on lanreotide Autogel
Abstract
Background: In acromegaly, expert surgery is curative in only about 60% of patients. Postoperative radiation therapy is associated with a high incidence of hypopituitarism and its effect on growth hormone (GH) production is slow, so that adjuvant medical treatment becomes of importance in the management of many patients.
Objective: To delineate the role of lanreotide in the treatment of acromegaly.
Methods: Search of Medline, Embase, and Web of Science databases for clinical studies of lanreotide in acromegaly.
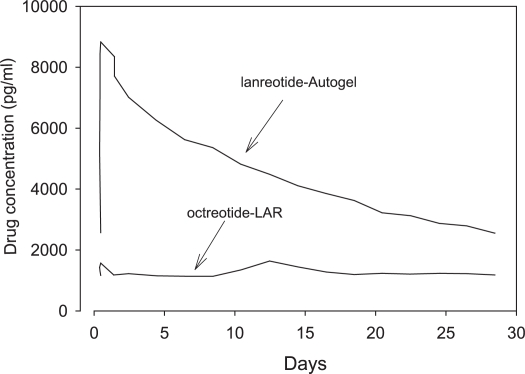
Results: Treatment with lanreotide slow release and lanreotide Autogel((R)) normalized GH and insulin-like growth factor-I (IGF-I) concentrations in about 50% of patients. The efficacy of 120 mg lanreotide Autogel((R)) on GH and IGF-I levels was comparable with that of 20 mg octreotide LAR. There were no differences in improvement of cardiac function, decrease in pancreatic beta-cell function, or occurrence of side effects, including cholelithiasis, between octreotide LAR and lanreotide Autogel(R). When postoperative treatment with somatostatin analogs does not result in normalization of serum IGF-I and GH levels after noncurative surgery, pegvisomant alone or in combination with somatostatin analogs can control these levels in a substantial number of patients.
Keywords: acromegaly; growth hormone; lanreotide; pegvisomant; somatostatin analog.
Figures
Similar articles
-
One-year follow-up of patients with acromegaly treated with fixed or titrated doses of lanreotide Autogel.Clin Endocrinol (Oxf). 2004 Jun;60(6):734-40. doi: 10.1111/j.1365-2265.2004.02045.x. Clin Endocrinol (Oxf). 2004. PMID: 15163338
-
Efficacy and tolerability of lanreotide Autogel therapy in acromegalic patients previously treated with octreotide LAR.Eur J Endocrinol. 2004 Sep;151(3):317-24. doi: 10.1530/eje.0.1510317. Eur J Endocrinol. 2004. PMID: 15362960 Clinical Trial.
-
Biochemical efficacy of long-acting lanreotide depot/Autogel in patients with acromegaly naïve to somatostatin-receptor ligands: analysis of three multicenter clinical trials.Pituitary. 2018 Jun;21(3):283-289. doi: 10.1007/s11102-018-0867-5. Pituitary. 2018. PMID: 29357081 Clinical Trial.
-
A critical analysis of clinically available somatostatin analog formulations for therapy of acromegaly.J Clin Endocrinol Metab. 2008 Aug;93(8):2957-68. doi: 10.1210/jc.2008-0027. Epub 2008 May 13. J Clin Endocrinol Metab. 2008. PMID: 18477663 Review.
-
Octreotide long-acting release (LAR): a review of its use in the management of acromegaly.Drugs. 2010 Sep 10;70(13):1745-69. doi: 10.2165/11204510-000000000-00000. Drugs. 2010. PMID: 20731479 Review.
Cited by
-
A New Approach to Supramolecular Structure Determination in Pharmaceutical Preparation of Self-Assembling Peptides: A Case Study of Lanreotide Autogel.Pharmaceutics. 2022 Mar 20;14(3):681. doi: 10.3390/pharmaceutics14030681. Pharmaceutics. 2022. PMID: 35336055 Free PMC article.
-
Direct palladium-mediated on-resin disulfide formation from Allocam protected peptides.Org Biomol Chem. 2017 Apr 5;15(14):2914-2918. doi: 10.1039/c7ob00536a. Org Biomol Chem. 2017. PMID: 28327729 Free PMC article.
-
Somatostatin receptor ligands in acromegaly: clinical response and factors predicting resistance.Pituitary. 2017 Feb;20(1):109-115. doi: 10.1007/s11102-016-0768-4. Pituitary. 2017. PMID: 27778296 Review.
-
Medical Treatment with Somatostatin Analogues in Acromegaly: Position Statement.Endocrinol Metab (Seoul). 2019 Mar;34(1):53-62. doi: 10.3803/EnM.2019.34.1.53. Endocrinol Metab (Seoul). 2019. PMID: 30912339 Free PMC article. Review.
-
Comparison of octreotide LAR and lanreotide autogel as post-operative medical treatment in acromegaly.Pituitary. 2012 Sep;15(3):398-404. doi: 10.1007/s11102-011-0335-y. Pituitary. 2012. PMID: 21863263 Free PMC article. Clinical Trial.
References
-
- Abe T, Lüdecke DK. Effects of preoperative octreotide treatment on different subtypes of 90 GH-secreting pituitary adenomas and outcome in one surgical centre. Eur J Endocrinol. 2001;145:137–45. - PubMed
-
- Abrams P, Alexopoulou O, Abs R, et al. Optimalization and cost management of lanreotide-Autogel therapy in acromegaly. Eur J Endocrinol. 2007;157:571–7. - PubMed
-
- Abs R, Verhelst J, Maiter D, et al. Cabergoline in the treatment of acromegaly: a study in 64 patients. J Clin Endocrinol Metab. 1998;83:374–8. - PubMed
-
- Ahmed S, Elsheikh M, Stratton IM, et al. Outcome of transsphenoidal surgery for acromegaly and its relationship to surgical experience. Clin Endocrinol (Oxf) 1999;50:561–7. - PubMed
-
- Alexander L, Appleton D, Hall R, et al. Epidemiology of acromegaly in the Newcastle region. Clin Endocrinol (Oxf) 1980;12:71–9. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
