

Biologic targeting in the treatment of inflammatory bowel diseases
- PMID: 19707398
- PMCID: PMC2726060
Biologic targeting in the treatment of inflammatory bowel diseases
Retraction in
-
Biologic targeting in the treatment of inflammatory bowel diseases [Retraction].Biologics. 2014 Jan 31;8:39. doi: 10.2147/BTT.S60301. eCollection 2014. Biologics. 2014. PMID: 24501538 Free PMC article. No abstract available.
Abstract
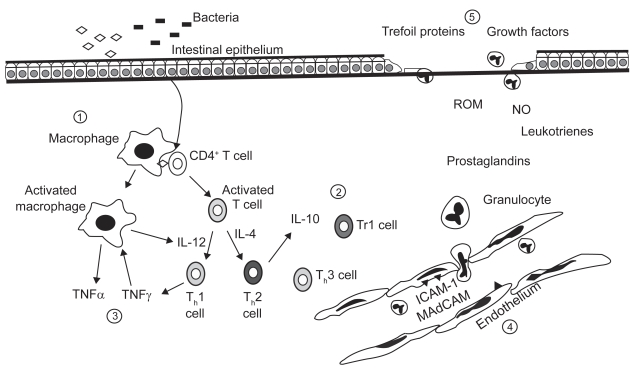
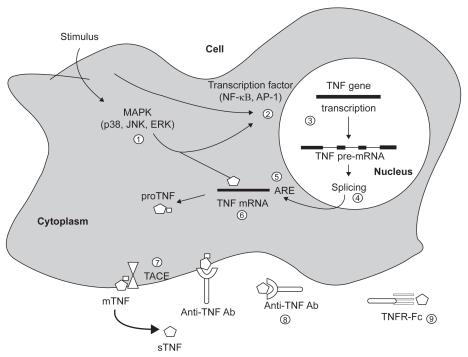
The etiology of inflammatory bowel disease (IBD) has not yet been clarified and immunosuppressive agents which nonspecifically reduce inflammation and immunity have been used in the conventional therapies for IBD. Evidence indicates that a dysregulation of mucosal immunity in the gut of IBD causes an overproduction of inflammatory cytokines and trafficking of effector leukocytes into the bowel, thus leading to an uncontrolled intestinal inflammation. Under normal situations, the intestinal mucosa is in a state of "controlled" inflammation regulated by a delicate balance of proinflammatory (tumor necrosis factor [TNF-alpha], interferon-gamma [IFN-gamma], interleukin-1 [IL-1], IL-6, IL-12 and anti-inflammatory cytokines IL-4, IL-10, IL-11). The mucosal immune system is the central effector of intestinal inflammation and injury, with cytokines playing a central role in modulating inflammation. Cytokines may therefore be a logical target for inflammatory bowel disease therapy using specific cytokine inhibitors. Biotechnology agents targeted against TNF, leukocyte adhesion, Th1 polarization, T cell activation, nuclear factor-kappaB (NF-kappaB), and other miscellaneous therapies are being evaluated as potential therapies for the treatment of inflammatory bowel disease. In this context, infliximab and adalimumab are currently the only biologic agents approved in Europe for the treatment of inflammatory Crohn's disease. Other anti-TNF biologic agents have emerged, including CDP571, certolizumab pegol, etanercept, onercept. However, ongoing research continues to generate new biologic agents targeted at specific pathogenic mechanism involved in the inflammatory process. Lymphocyte-endothelial interactions mediated by adhesion molecules are important in leukocyte migration and recruitment to sites of inflammation, and selective blockade of these adhesion molecules is a novel and promising strategy to treat Crohn's disease. Therapeutics agents to inhibit leukocyte trafficking include natalizumab (approved for use in Crohn's disease in USA), MLN-02, and ISIS 2302. Other agents being investigated for the treatment of Crohn's disease include inhibitors of T cell activation, proinflammatory cytokine receptors, Th1 polarization, growth hormone, and growth factors. Agents being investigated for treatment of ulcerative colitis include many of those mentioned above. Controlled clinical trials are currently being conducted, exploring the safety and efficacy of old and new biologic agents, and the search certainly will open new and exciting perspective on the development of therapies for inflammatory bowel disease. A review is made of the main areas of research exploring the mechanisms associated with the pathogenesis of IBD, providing advances in the agents currently in use, and identifying a host of new therapeutic biologic targets.
Keywords: Crohn’s disease; biological therapy; ulcerative colitis.
Figures
References
-
- van Assche G. Emerging drugs to treat Crohn’s disease. Expert Opin Emerging Drugs. 2007;12:49–59. - PubMed
-
- Hanauer SB, Present DH. The state of the art in the management of inflammatory bowel disease. Rev Gastroenterol Disord. 2003;3:81–92. - PubMed
-
- Hanauer SB, Sandborn WJ. Practice Parameters Committee of the American College of Gastroenterology. Management of Crohn’s disease in adults. Am J Gastroenterol. 2001;96:635–643. - PubMed
-
- Sandborn WJ, Feagan BG. Review article: mild to moderate Crohn’s disease- defining the basis for a new treatment algorithm. Aliment Pharmacol Ther. 2003;18:263–277. - PubMed
-
- Camma’ C, Giunta M, Rosselli M, et al. Mesalamine in the maintenance treatment of Crohn’s disease: a meta-analysis adjusted for confounding variables. Gastroenterology. 1997;113:1465–1473. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
