

4-D cardiac MR image analysis: left and right ventricular morphology and function
- PMID: 19709962
- PMCID: PMC2849009
- DOI: 10.1109/TMI.2009.2030799
4-D cardiac MR image analysis: left and right ventricular morphology and function
Abstract
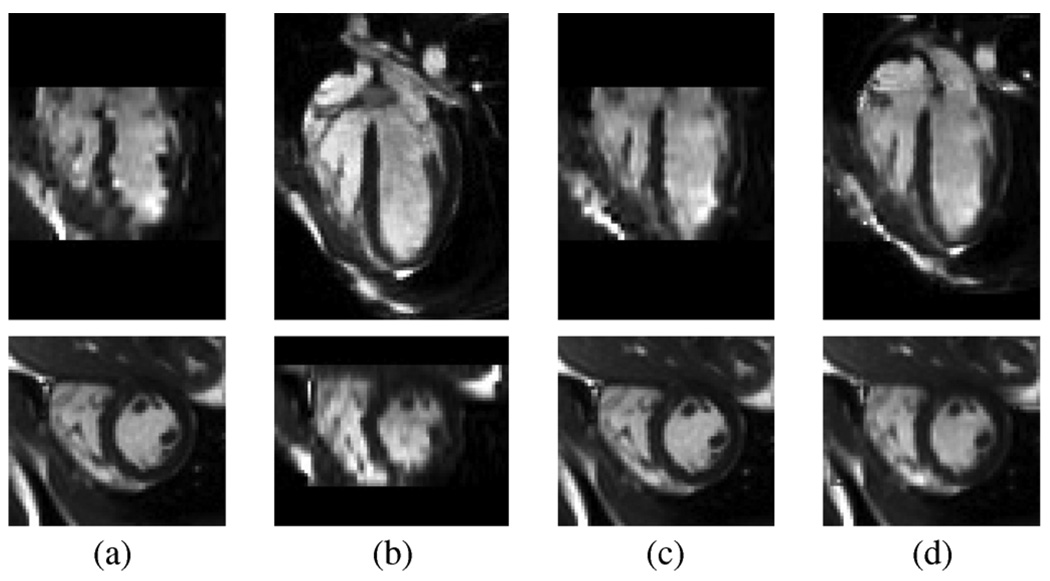
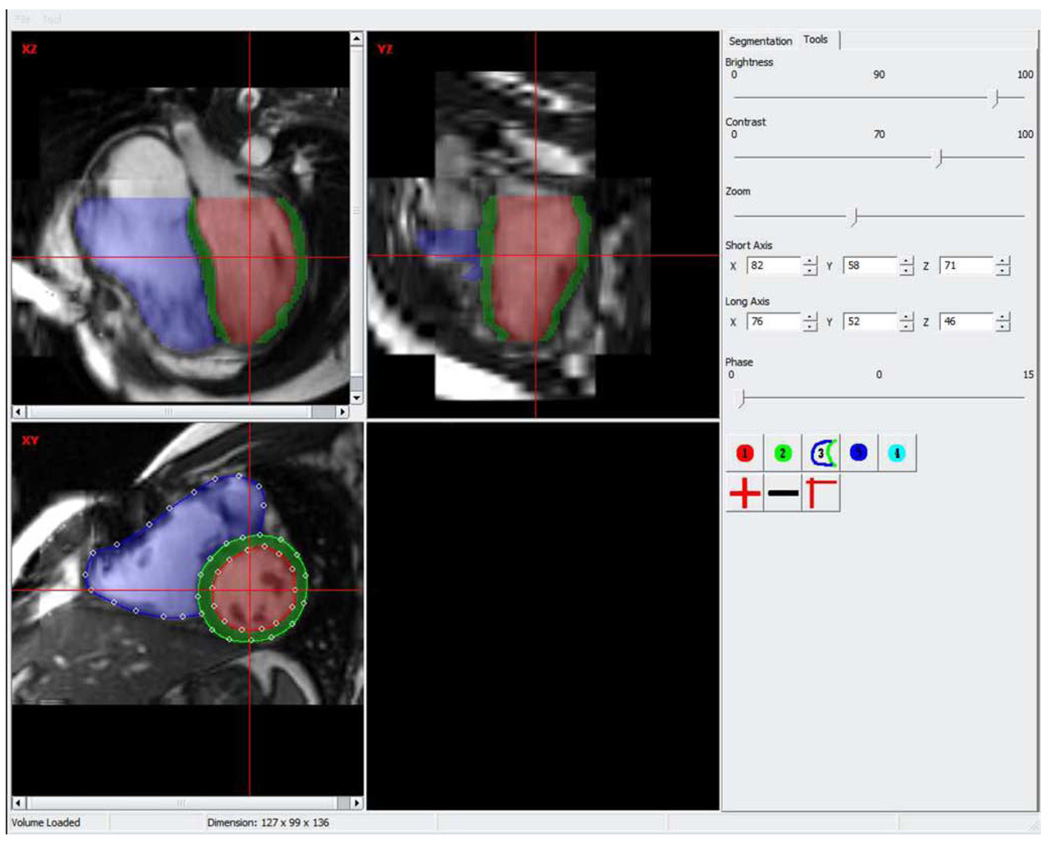
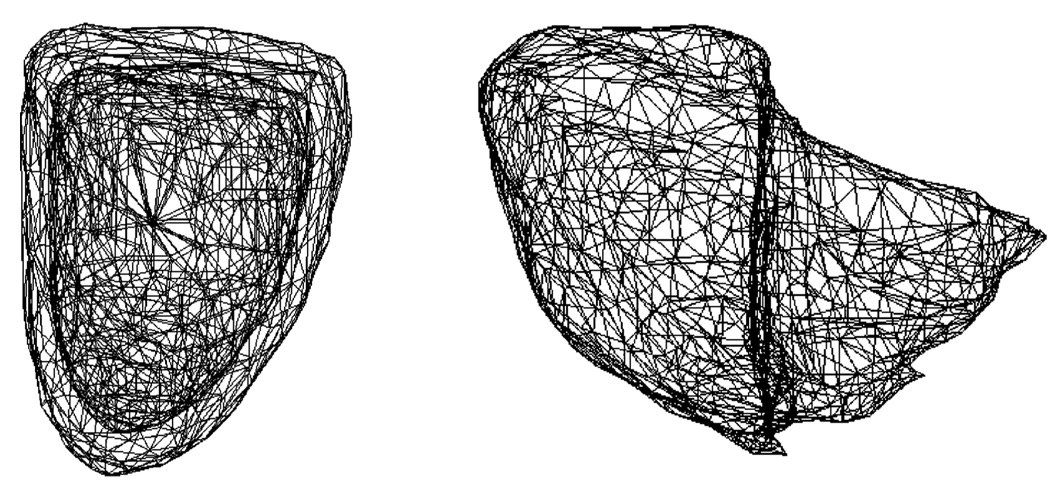
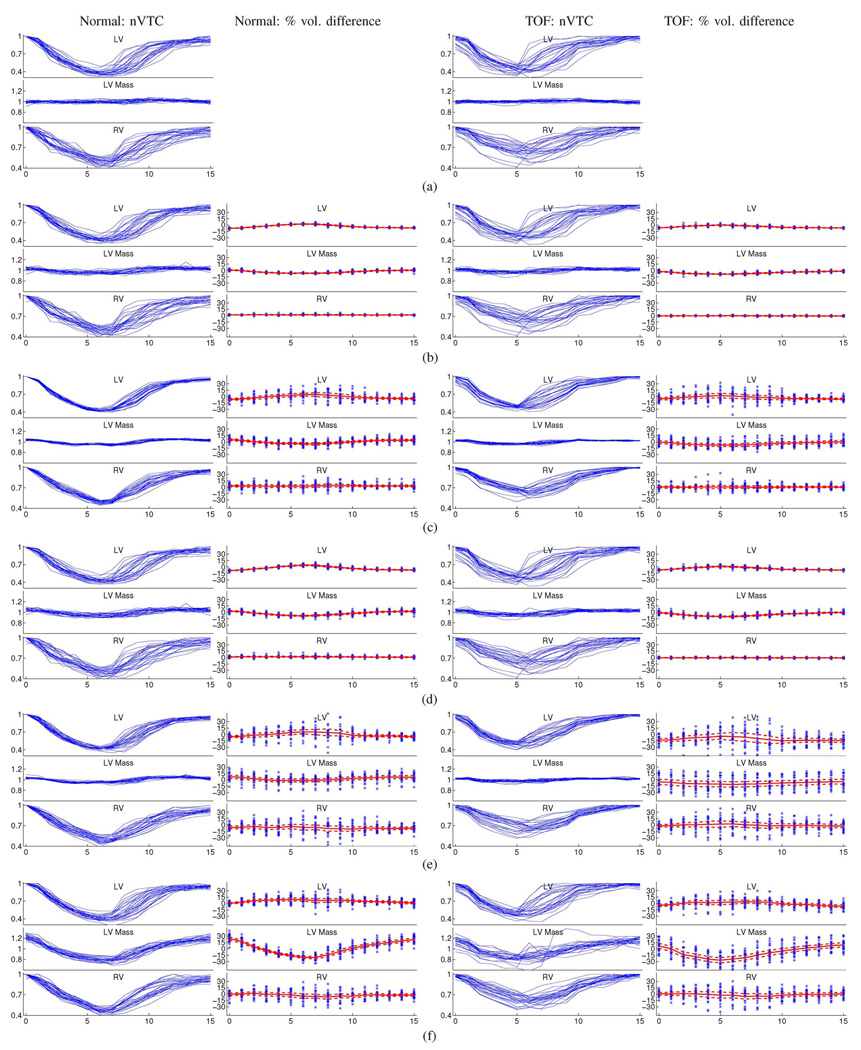
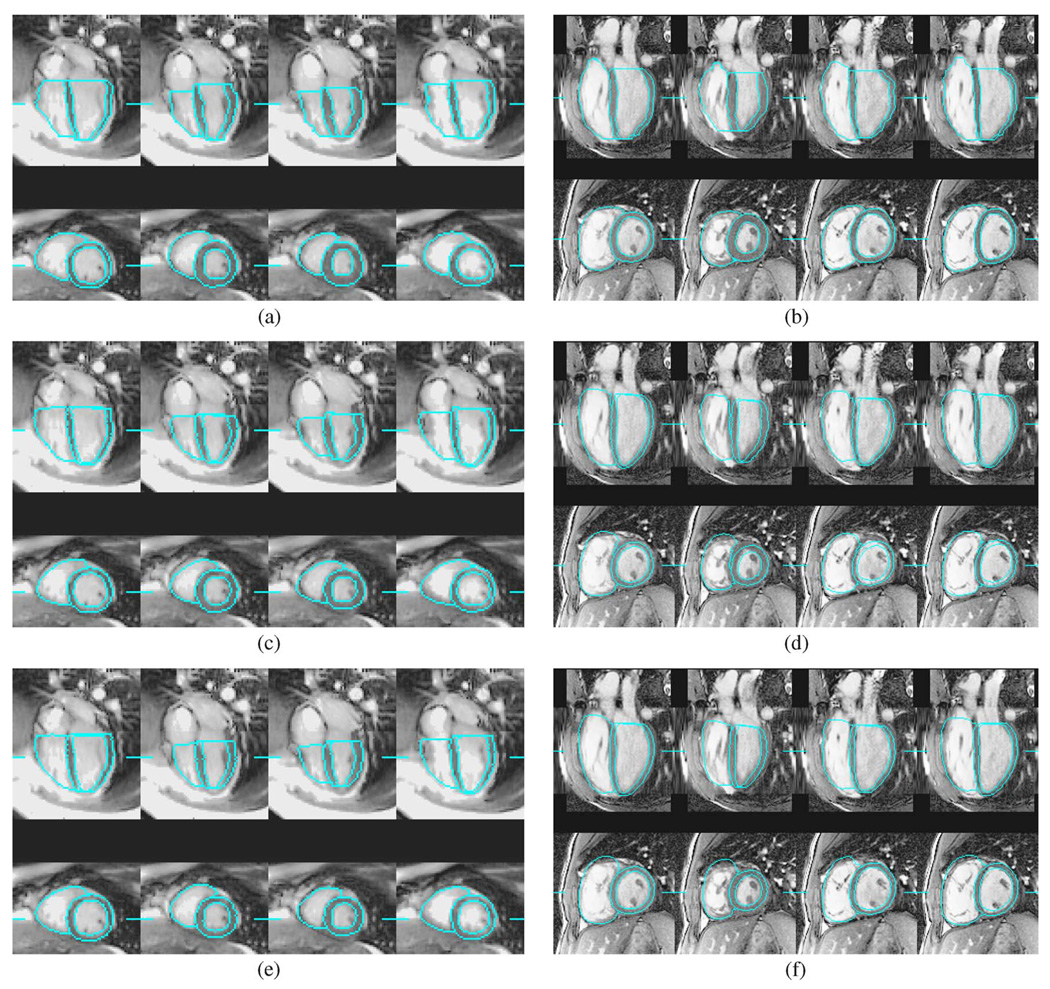
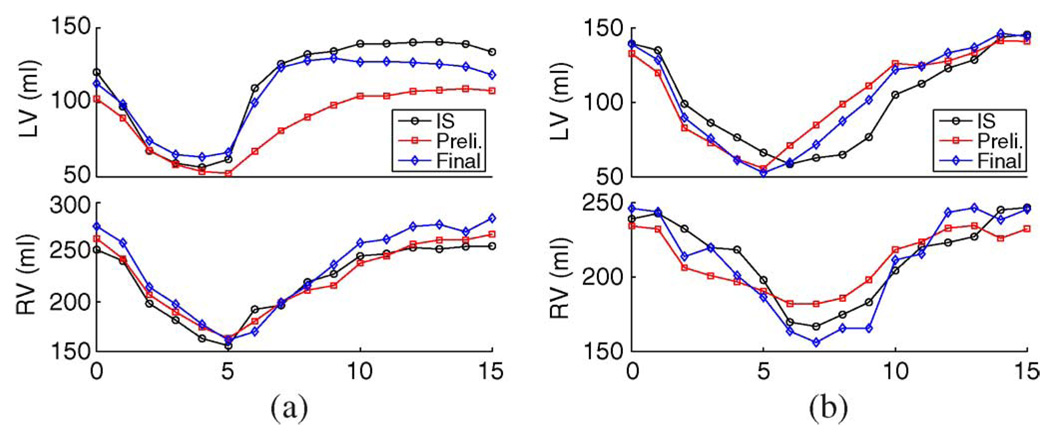
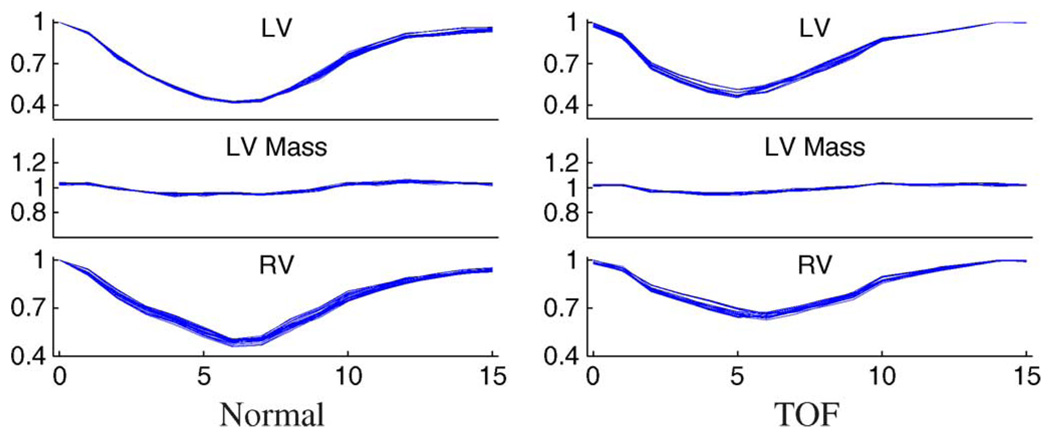
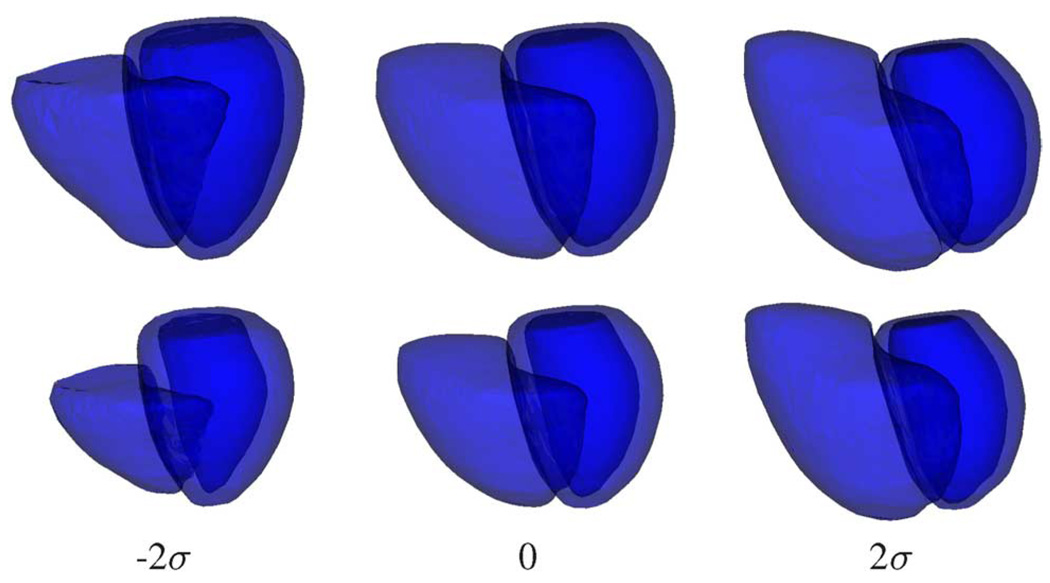
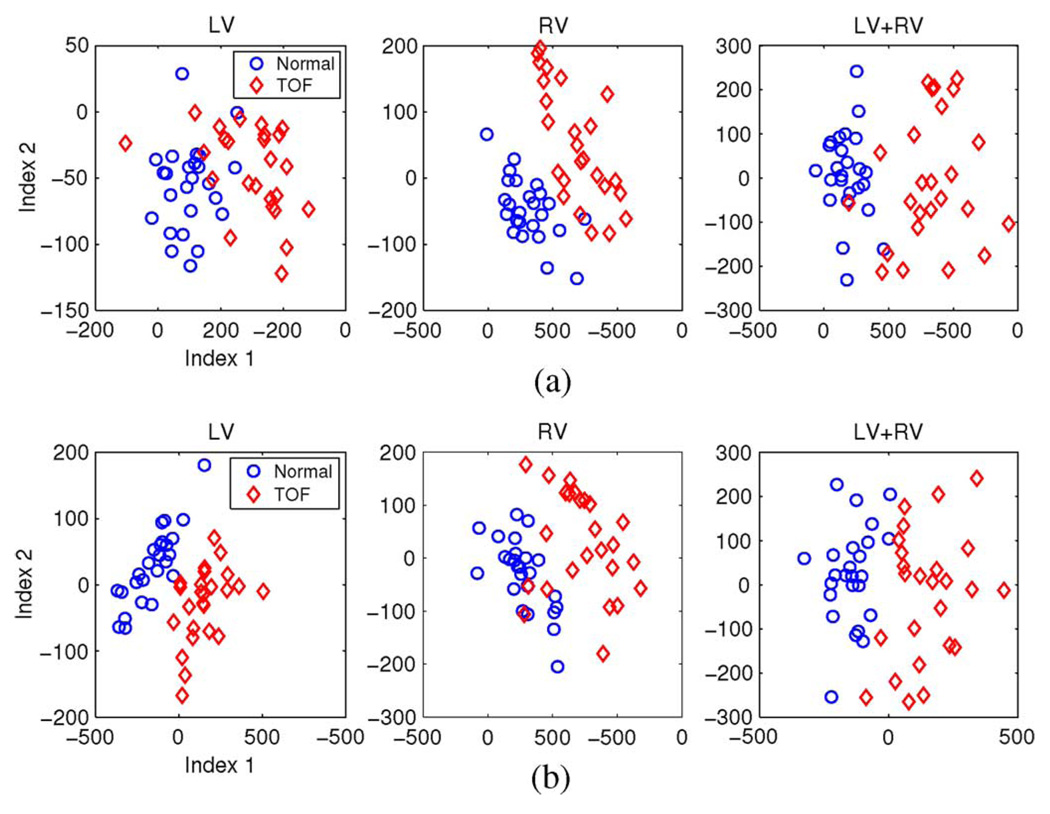
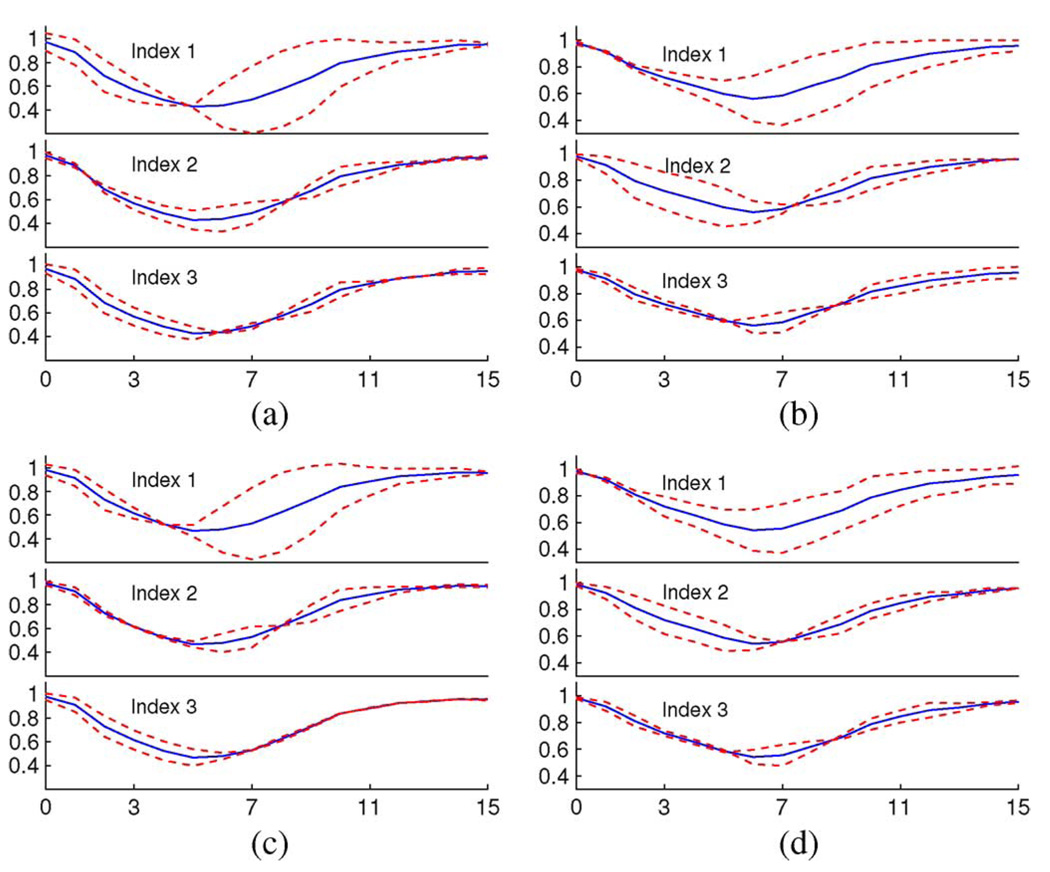
In this study, a combination of active shape model (ASM) and active appearance model (AAM) was used to segment the left and right ventricles of normal and Tetralogy of Fallot (TOF) hearts on 4-D (3-D+time) MR images. For each ventricle, a 4-D model was first used to achieve robust preliminary segmentation on all cardiac phases simultaneously and a 3-D model was then applied to each phase to improve local accuracy while maintaining the overall robustness of the 4-D segmentation. On 25 normal and 25 TOF hearts, in comparison to the expert traced independent standard, our comprehensive performance assessment showed subvoxel segmentation accuracy, high overlap ratios, good ventricular volume correlations, and small percent volume differences. Following 4-D segmentation, novel quantitative shape and motion features were extracted using shape information, volume-time and dV/dt curves, analyzed and used for disease status classification. Automated discrimination between normal/TOF subjects achieved 90%-100% sensitivity and specificity. The features obtained from TOF hearts show higher variability compared to normal subjects, suggesting their potential use as disease progression indicators. The abnormal shape and motion variations of the TOF hearts were accurately captured by both the segmentation and feature characterization.
Figures

References
-
- Anderson RH, Tynan M. Tetralogy of Fallot—A centennial review. Int. J. Cardiol. 1988 Dec;vol. 21(no. 3):219–232. - PubMed
-
- Gatzoulis MA, Webb GD, Daubeney PEF. Diagnosis and Management of Adult Congenital Heart Disease. New York: Churchill Livingstone; 2003.
-
- Anderson RH, Weinberg PM. The clinical anatomy of tetralogy of Fallot. Cardiol. Young. 2005 Feb;vol. 15(no. 1):38–47. - PubMed
-
- Hoffman JIE, Kaplan S, Liberthson RR. Prevalence of congenital heart disease. Am. Heart J. 2004 Mar;vol. 147(no. 3):425–439. - PubMed
-
- Helbing WA, de Roos A. Clinical applications of cardiac magnetic resonance imaging after repair of tetralogy of Fallot. Pediatr. Cardiol. 2000;vol. 21(no. 1):70–79. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
