

Intra-tubular deposits, urine and stone composition are divergent in patients with ileostomy
- PMID: 19710630
- PMCID: PMC3780771
- DOI: 10.1038/ki.2009.321
Intra-tubular deposits, urine and stone composition are divergent in patients with ileostomy
Abstract
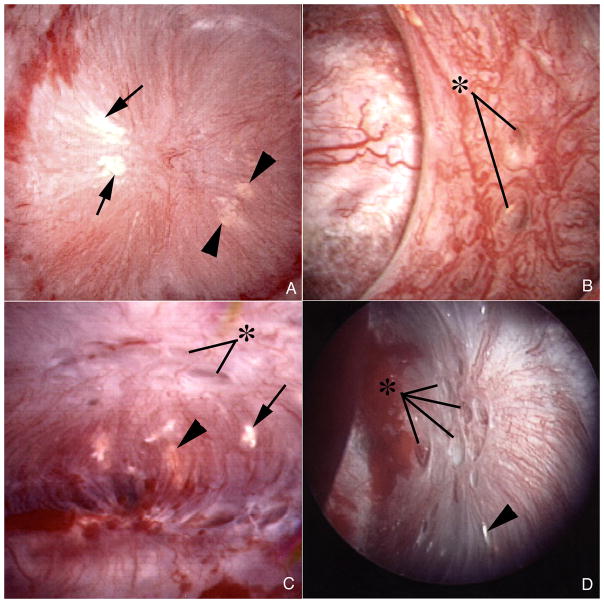
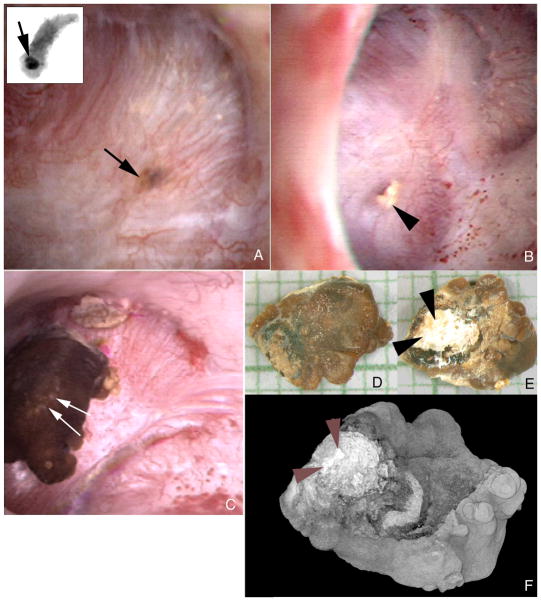
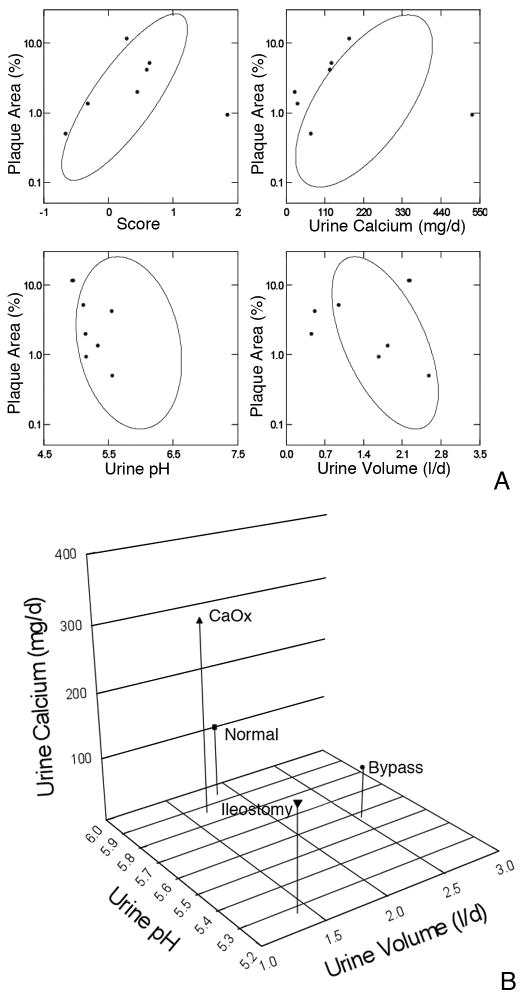
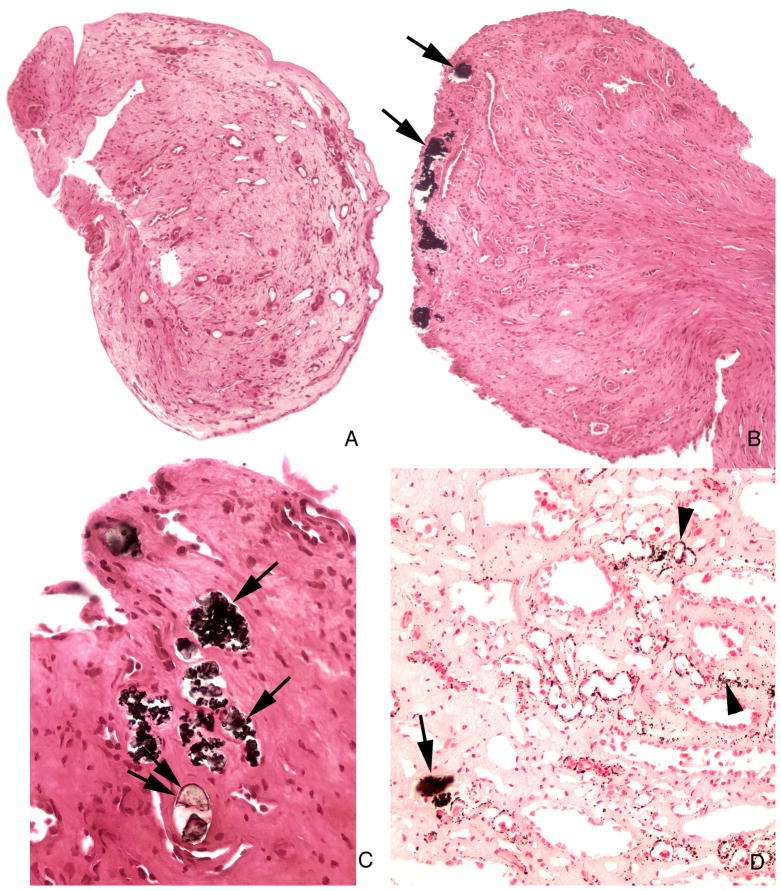
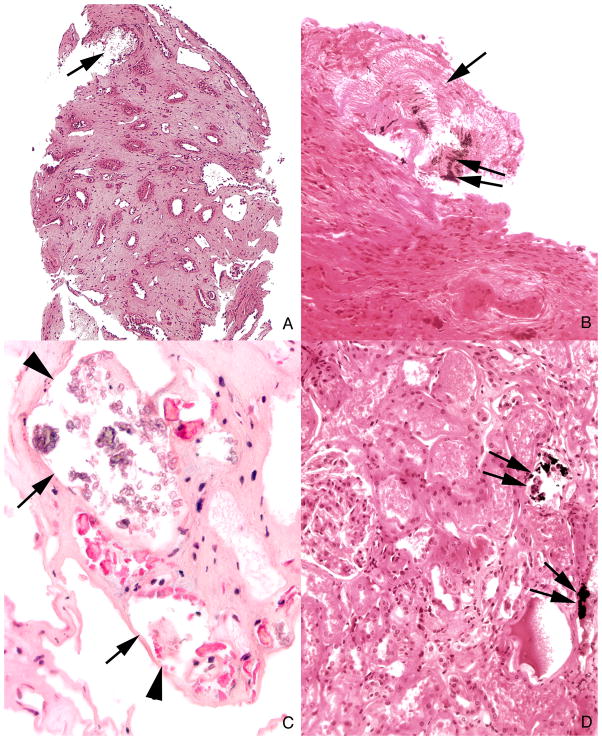
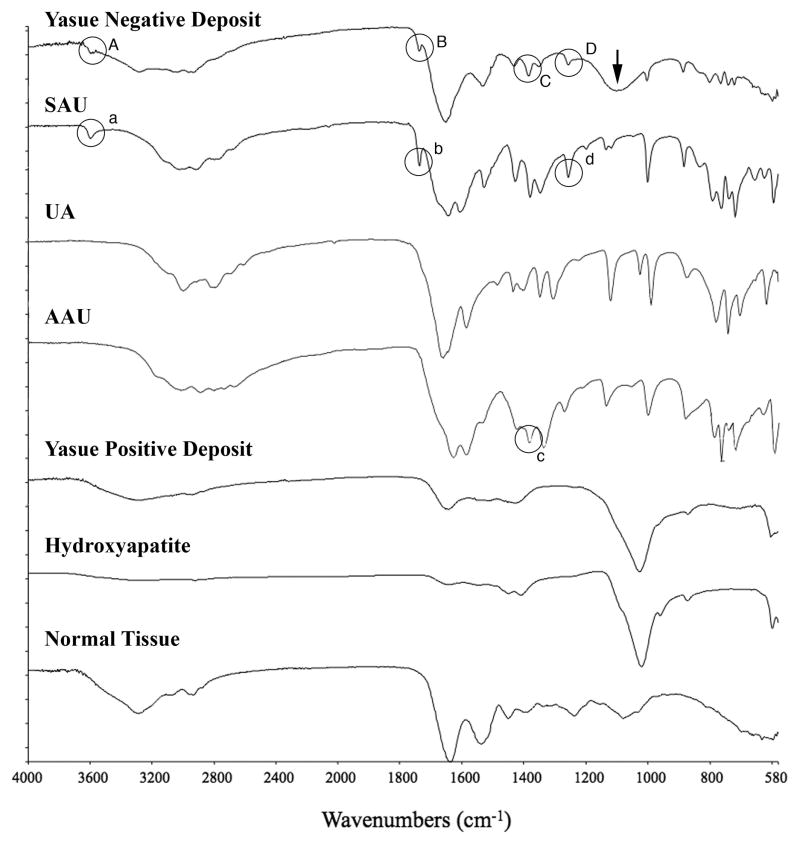
Patients with ileostomy typically have recurrent renal stones and produce scanty, acidic, sodium-poor urine because of abnormally large enteric losses of water and sodium bicarbonate. Here we used a combination of intra-operative digital photography and biopsy of the renal papilla and cortex to measure changes associated with stone formation in seven patients with ileostomy. Papillary deformity was present in four patients and was associated with decreased estimated glomerular filtration rates. All patients had interstitial apatite plaque, as predicted from their generally acid, low-volume urine. Two patients had stones attached to plaque; however, all patients had crystal deposits that plugged the ducts of Bellini and inner medullary collecting ducts (IMCDs). Despite acid urine, all crystal deposits contained apatite, and five patients had deposits of sodium and ammonium acid urates. Stones were either uric acid or calcium oxalate as predicted by supersaturation, however, there was a general lack of supersaturation for calcium phosphate as brushite, sodium, or ammonium acid urate because of the overall low urine pH. This suggests that local tubular pH exceeds that of bulk urine. Despite low urine pH, patients with an ileostomy resemble those with obesity bypass, in whom IMCD apatite crystal plugs are found. They are, however, unlike these bypass patients in having interstitial apatite plaque. IMCD plugging with sodium and ammonium acid urate has not been found previously and appears to correlate with formation of uric acid stones.
Conflict of interest statement
The authors have no interests to disclose relevant to this publication.
Figures
References
-
- Clarke AM, Chirnside A, Hill GL, et al. Chronic dehydration and sodium depletion in patients with established ileostonies. Lancet. 1967;2:740–743. - PubMed
-
- Worcester EM. Stones due to bowel disease. In: Coe FL, Favus MJ, Pak CY, et al., editors. Kidney Stones: Medical and Surgical Management. chap 39. Philadelphia: Lippincott-Raven; 1996. pp. 883–903.
-
- Parks JH, Worcester EM, O’Connor RC, Coe FL. Urine stone risk factors in nephrolithiasis patients with and without bowel disease. Kidney Int. 2003;63:255–265. - PubMed
-
- Randall RE. Urate nephropathy following chronic ileostomy acidosis. Am J Nephrol. 2002;22:372–375. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
