

Glucose absorption and gastric emptying in critical illness
- PMID: 19712450
- PMCID: PMC2750198
- DOI: 10.1186/cc8021
Glucose absorption and gastric emptying in critical illness
Abstract
Introduction: Delayed gastric emptying occurs frequently in critically ill patients and has the potential to adversely affect both the rate, and extent, of nutrient absorption. However, there is limited information about nutrient absorption in the critically ill, and the relationship between gastric emptying (GE) and absorption has hitherto not been evaluated. The aim of this study was to quantify glucose absorption and the relationships between GE, glucose absorption and glycaemia in critically ill patients.
Methods: Studies were performed in nineteen mechanically-ventilated critically ill patients and compared to nineteen healthy subjects. Following 4 hours fasting, 100 ml of Ensure, 2 g 3-O-methyl glucose (3-OMG) and 99mTc sulphur colloid were infused into the stomach over 5 minutes. Glucose absorption (plasma 3-OMG), blood glucose levels and GE (scintigraphy) were measured over four hours. Data are mean +/- SEM. A P-value < 0.05 was considered significant.
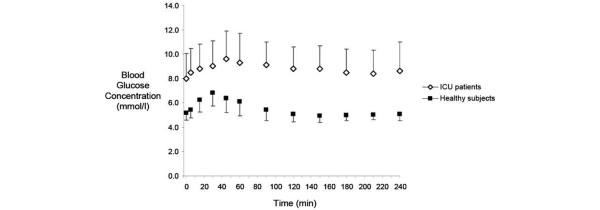
Results: Absorption of 3-OMG was markedly reduced in patients (AUC240: 26.2 +/- 18.4 vs. 66.6 +/- 16.8; P < 0.001; peak: 0.17 +/- 0.12 vs. 0.37 +/- 0.098 mMol/l; P < 0.001; time to peak; 151 +/- 84 vs. 89 +/- 33 minutes; P = 0.007); and both the baseline (8.0 +/- 2.1 vs. 5.6 +/- 0.23 mMol/l; P < 0.001) and peak (10.0 +/- 2.2 vs. 7.7 +/- 0.2 mMol/l; P < 0.001) blood glucose levels were higher in patients; compared to healthy subjects. In patients; 3-OMG absorption was directly related to GE (AUC240; r = -0.77 to -0.87; P < 0.001; peak concentrations; r = -0.75 to -0.81; P = 0.001; time to peak; r = 0.89-0.94; P < 0.001); but when GE was normal (percent retention240 < 10%; n = 9) absorption was still impaired. GE was inversely related to baseline blood glucose, such that elevated levels were associated with slower GE (ret 60, 180 and 240 minutes: r > 0.51; P < 0.05).
Conclusions: In critically ill patients; (i) the rate and extent of glucose absorption are markedly reduced; (ii) GE is a major determinant of the rate of absorption, but does not fully account for the extent of impaired absorption; (iii) blood glucose concentration could be one of a number of factors affecting GE.
Figures



Comment in
-
Impaired glucose and nutrient absorption in critical illness: is gastric emptying only a piece of the puzzle?Crit Care. 2009;13(5):190. doi: 10.1186/cc8049. Epub 2009 Oct 1. Crit Care. 2009. PMID: 19818163 Free PMC article.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
