

Has payment by results affected the way that English hospitals provide care? Difference-in-differences analysis
- PMID: 19713233
- PMCID: PMC2733950
- DOI: 10.1136/bmj.b3047
Has payment by results affected the way that English hospitals provide care? Difference-in-differences analysis
Abstract
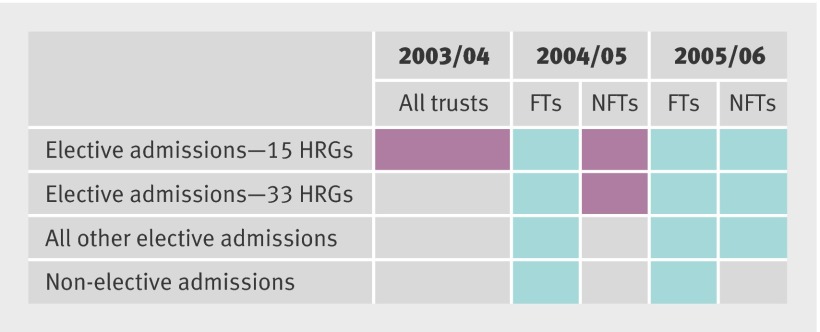
Objective: To examine whether the introduction of payment by results (a fixed tariff case mix based payment system) was associated with changes in key outcome variables measuring volume, cost, and quality of care between 2003/4 and 2005/6.
Setting: Acute care hospitals in England.
Design: Difference-in-differences analysis (using a control group created from trusts in England and providers in Scotland not implementing payment by results in the relevant years); retrospective analysis of patient level secondary data with fixed effects models.
Data sources: English hospital episode statistics and Scottish morbidity records for 2002/3 to 2005/6.
Main outcome measures: Changes in length of stay and proportion of day case admissions as a proxy for unit cost; growth in number of spells to measure increases in output; and changes in in-hospital mortality, 30 day post-surgical mortality, and emergency readmission after treatment for hip fracture as measures of impact on quality of care.
Results: Length of stay fell more quickly and the proportion of day cases increased more quickly where payment by results was implemented, suggesting a reduction in the unit costs of care associated with payment by results. Some evidence of an association between the introduction of payment by results and growth in acute hospital activity was found. Little measurable change occurred in the quality of care indicators used in this study that can be attributed to the introduction of payment by results.
Conclusion: Reductions in unit costs may have been achieved without detrimental impact on the quality of care, at least in as far as these are measured by the proxy variables used in this study.
Conflict of interest statement
Competing interests: None declared.
Figures
Comment in
-
The effects of payment by results.BMJ. 2009 Aug 27;339:b3081. doi: 10.1136/bmj.b3081. BMJ. 2009. PMID: 19713234 No abstract available.
-
Payment by results. Market failure.BMJ. 2009 Sep 22;339:b3859. doi: 10.1136/bmj.b3859. BMJ. 2009. PMID: 19773314 No abstract available.
References
-
- Department of Health. Reforming NHS financial flows: introducing payment by results. London: Department of Health, 2002.
-
- Sussex J, Street A. Activity-based financing for hospitals: English policy and international experience. London: Office of Health Economics, 2005.
-
- Department of Health. NHS reference costs 2003 and national tariff 2004 (payment by results core tools 2004). London: Department of Health, 2004.
-
- Raftery J, Robinson R, Mulligan J, Forrest S. Contracting in the NHS quasi-market. Health Econ 1996;5:353-62. - PubMed
-
- Chalkley M, Malcolmson JM. Government purchasing of health services. In: Culyer AJ, Newhouse JP, eds. Handbook of health economics. Vol 1A. Amsterdam: North-Holland, 2000:847-90.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical