

Bone marrow stromal cells attenuate lung injury in a murine model of neonatal chronic lung disease
- PMID: 19713447
- PMCID: PMC2784417
- DOI: 10.1164/rccm.200902-0242OC
Bone marrow stromal cells attenuate lung injury in a murine model of neonatal chronic lung disease
Abstract
Rationale: Neonatal chronic lung disease, known as bronchopulmonary dysplasia (BPD), remains a serious complication of prematurity despite advances in the treatment of extremely low birth weight infants.
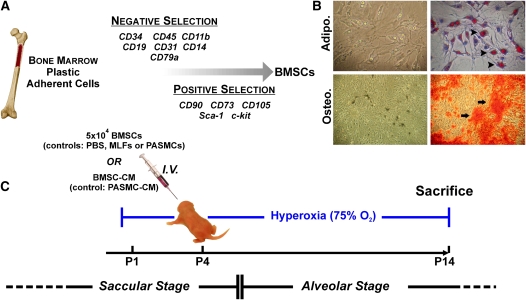
Objectives: Given the reported protective actions of bone marrow stromal cells (BMSCs; mesenchymal stem cells) in models of lung and cardiovascular injury, we tested their therapeutic potential in a murine model of BPD.
Methods: Neonatal mice exposed to hyperoxia (75% O(2)) were injected intravenously on Day 4 with either BMSCs or BMSC-conditioned media (CM) and assessed on Day 14 for lung morphometry, vascular changes associated with pulmonary hypertension, and lung cytokine profile.
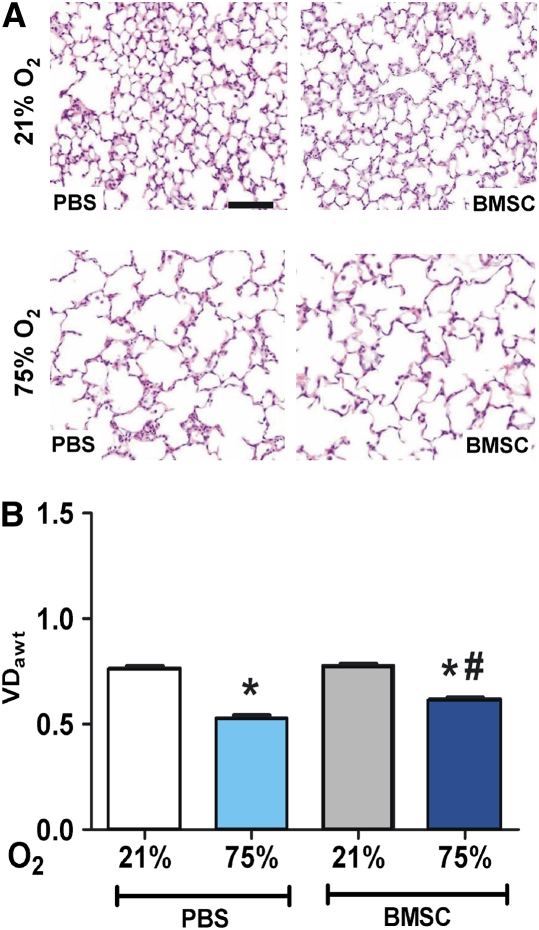
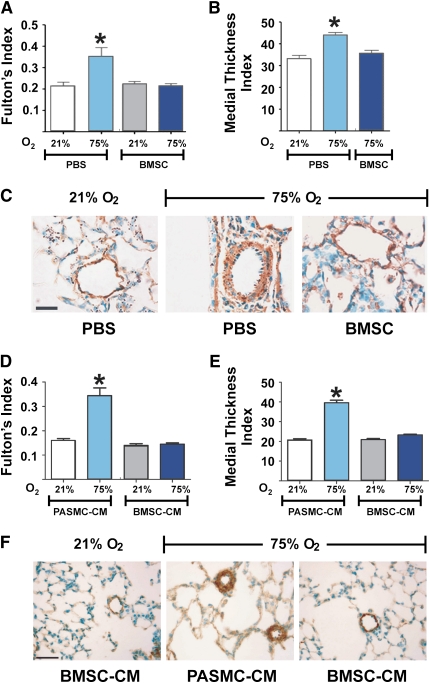
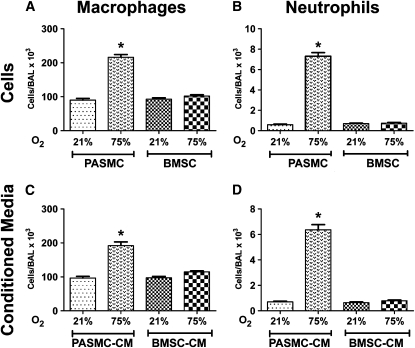
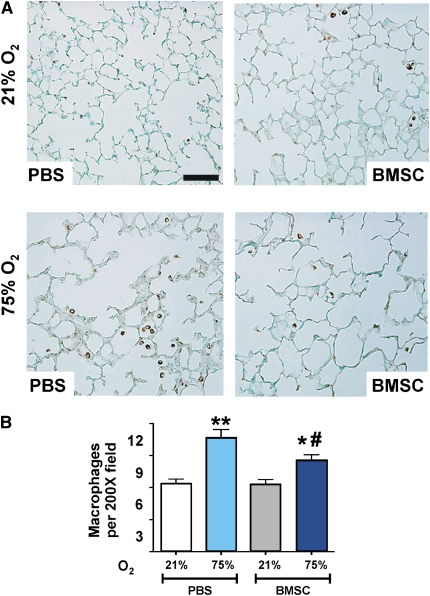
Measurements and main results: Injection of BMSCs but not pulmonary artery smooth muscle cells (PASMCs) reduced alveolar loss and lung inflammation, and prevented pulmonary hypertension. Although more donor BMSCs engrafted in hyperoxic lungs compared with normoxic controls, the overall low numbers suggest protective mechanisms other than direct tissue repair. Injection of BMSC-CM had a more pronounced effect than BMSCs, preventing both vessel remodeling and alveolar injury. Treated animals had normal alveolar numbers at Day 14 of hyperoxia and a drastically reduced lung neutrophil and macrophage accumulation compared with PASMC-CM-treated controls. Macrophage stimulating factor 1 and osteopontin, both present at high levels in BMSC-CM, may be involved in this immunomodulation.
Conclusions: BMSCs act in a paracrine manner via the release of immunomodulatory factors to ameliorate the parenchymal and vascular injury of BPD in vivo. Our study suggests that BMSCs and factor(s) they secrete offer new therapeutic approaches for lung diseases currently lacking effective treatment.
Figures

Comment in
-
Mesenchymal stem cells for the prevention of bronchopulmonary dysplasia: delivering the secretome.Am J Respir Crit Care Med. 2009 Dec 1;180(11):1039-41. doi: 10.1164/rccm.200909-1330ED. Am J Respir Crit Care Med. 2009. PMID: 19923401 No abstract available.
References
-
- Kinsella JP, Greenough A, Abman SH. Bronchopulmonary dysplasia. Lancet 2006;367:1421–1431. - PubMed
-
- Stenmark KR, Abman SH. Lung vascular development: implications for the pathogenesis of bronchopulmonary dysplasia. Annu Rev Physiol 2005;67:623–661. - PubMed
-
- Abman SH. Pulmonary hypertension in chronic lung disease of infancy. Pathogenesis, pathophysiology and treatment. In: Bland RD, Coalson JJ, editors. Chronic lung disease of infancy. New York: Marcel Dekker; 2000. pp. 619–668.
-
- Baveja R, Christou H. Pharmacological strategies in the prevention and management of bronchopulmonary dysplasia. Semin Perinatol 2006;30:209–218. - PubMed
-
- Pereira RF, O'Hara MD, Laptev AV, Halford KW, Pollard MD, Class R, Simon D, Livezey K, Prockop DJ. Marrow stromal cells as a source of progenitor cells for nonhematopoietic tissues in transgenic mice with a phenotype of osteogenesis imperfecta. Proc Natl Acad Sci USA 1998;95:1142–1147. - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
