

Something old or something new? Social health insurance in Ghana
- PMID: 19715583
- PMCID: PMC2739838
- DOI: 10.1186/1472-698X-9-20
Something old or something new? Social health insurance in Ghana
Abstract
Background: There is considerable interest at present in exploring the potential of social health insurance to increase access to and affordability of health care in Africa. A number of countries are currently experimenting with different approaches. Ghana's National Health Insurance Scheme (NHIS) was passed into law in 2003 but fully implemented from late 2005. It has already reached impressive coverage levels. This article aims to provide a preliminary assessment of the NHIS to date. This can inform the development of the NHIS itself but also other innovations in the region.
Methods: This article is based on analysis of routine data, on secondary literature and on key informant interviews conducted by the authors with stakeholders at national, regional and district levels over the period of 2005 to 2009.
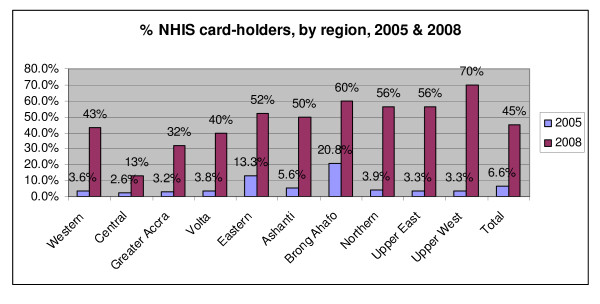
Results: In relation to its financing sources, the NHIS is heavily reliant on tax funding for 70-75% of its revenue. This has permitted quick expansion of coverage, partly through the inclusion of large exempted population groups. Card holders increased from 7% of the population in 2005 to 45% in 2008. However, only around a third of these are contributing to the scheme financially. This presents a sustainability problem, in that revenue is de-coupled from the growing membership. In addition, the NHIS offers a broad benefits package, with no co-payments and limited gate-keeping, and also faces cost escalation related to its new payment system and the growing utilisation of members. These features contributed to a growth in distressed schemes and failure to pay outstanding facility claims in 2008.The NHIS has had a considerable impact on the health system as a whole, taking on a growing role in funding curative care. In 2009, it is expected to contribute 41% of the overall resource envelope. However there is evidence that this funding is not additional but has been switched from other funding channels. There are some equity concerns about this, as the new funding source (a VAT-based tax) may be more regressive. In addition, membership of the NHIS at present has a pro-rich bias, and a pro-urban bias in relation to renewals. Only a very small proportion is registered as indigent, and there is some evidence of 'squeezing out' of non-members from health care utilisation. Finally, considerable challenges remain in relation to strengthening the purchasing role of the NHIS, and also settling debates about its structure and accountability.
Conclusion: Some trade-offs will be necessary between the existing wide benefits package of the NHIS and the laudable desire to reach universal coverage. The overall resource envelope for health is likely to be stable rather than increasing over the medium-term. In the longer term, the investment costs in the NHIS will only be justified if it is able to increase the cost-effectiveness of purchasing and the responsiveness of the system as a whole.
Figures
References
-
- World Health Organisation. Moving Towards Universal Coverage Series. Geneva, WHO; 2006.
-
- Carrin G, Doetinchem O, Kirigia J, Mathauer I, Musango L. Social health insurance: how feasible is its expansion in the African region? DevISSues. 2008. http://www.iss.nl/layout/set/print/content/view/full/12939
LinkOut - more resources
Full Text Sources
