

Endovascular treatment with angioplasty or stenting versus endarterectomy in patients with carotid artery stenosis in the Carotid and Vertebral Artery Transluminal Angioplasty Study (CAVATAS): long-term follow-up of a randomised trial
- PMID: 19717345
- PMCID: PMC2755037
- DOI: 10.1016/S1474-4422(09)70228-5
Endovascular treatment with angioplasty or stenting versus endarterectomy in patients with carotid artery stenosis in the Carotid and Vertebral Artery Transluminal Angioplasty Study (CAVATAS): long-term follow-up of a randomised trial
Abstract
Background: Endovascular treatment (angioplasty with or without stenting) is an alternative to carotid endarterectomy for carotid artery stenosis but there are scarce long-term efficacy data showing that it prevents stroke. We therefore report the long-term results of the Carotid and Vertebral Artery Transluminal Angioplasty Study (CAVATAS).
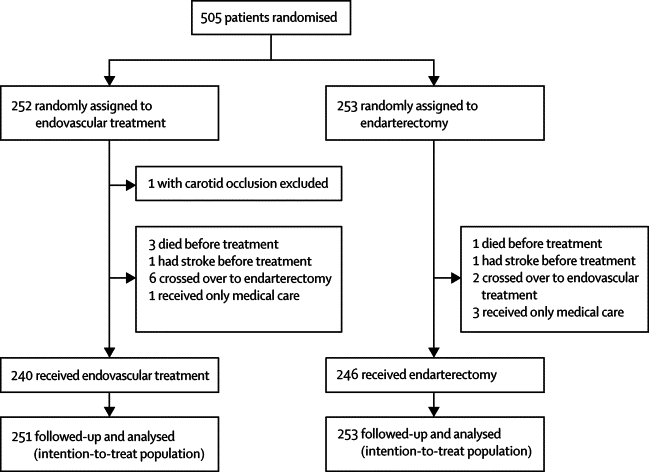
Methods: Between March, 1992, and July, 1997, patients who presented at a participating centre with a confirmed stenosis of the internal carotid artery that was deemed equally suitable for either carotid endarterectomy or endovascular treatment were randomly assigned to either treatment in equal proportions by telephone or fax from the randomisation service at the Oxford Clinical Trials Unit, UK. Patients were seen by an independent neurologist at 1 and 6 months after treatment and then every year after randomisation for as long as possible, up to a maximum of 11 years. Major outcome events were transient ischaemic attack, non-disabling, disabling, and fatal stroke, myocardial infarction, and death from any other cause. Outcomes were adjudicated on by investigators who were masked to treatment. Analysis was by intention to treat. This study is registered, number ISRCTN 01425573.
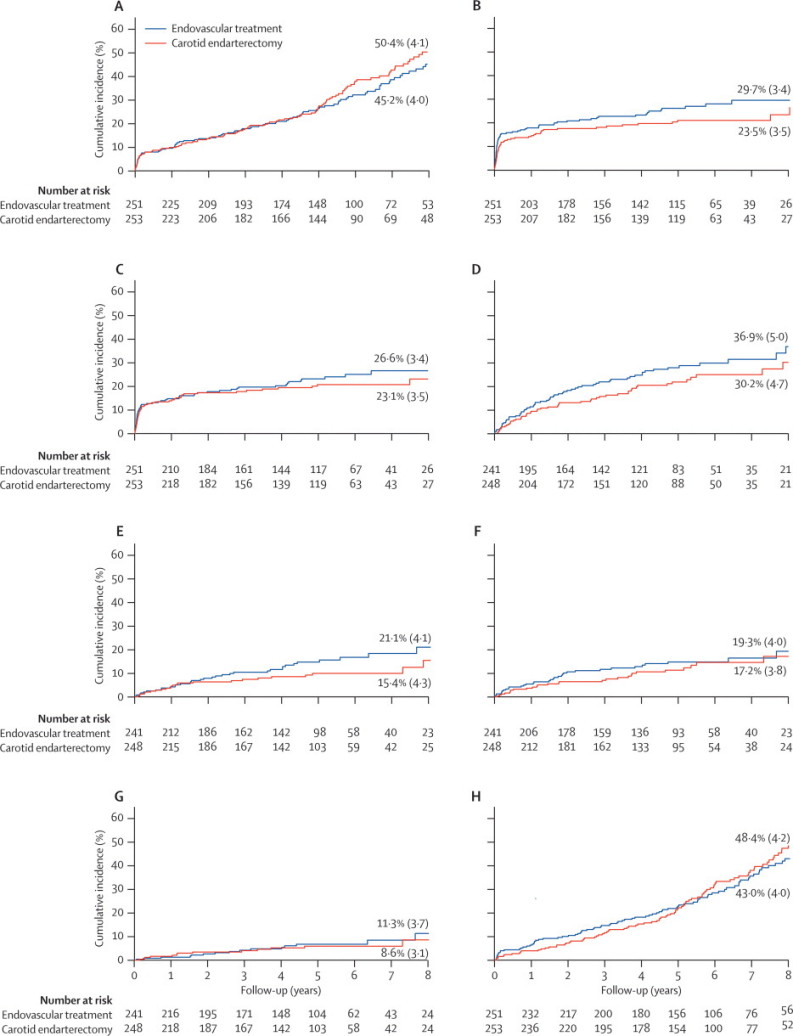
Findings: 504 patients with stenosis of the carotid artery (90% symptomatic) were randomly assigned to endovascular treatment (n=251) or surgery (n=253). Within 30 days of treatment, there were more minor strokes that lasted less than 7 days in the endovascular group (8 vs 1) but the number of other strokes in any territory or death was the same (25 vs 25). There were more cranial nerve palsies (22 vs 0) in the endarterectomy group than in the endovascular group. Median length of follow up in both groups was 5 years (IQR 2-6). By comparing endovascular treatment with endarterectomy after the 30-day post-treatment period, the 8-year incidence and hazard ratio (HR) at the end of follow-up for ipsilateral non-perioperative stroke was 11.3% versus 8.6% (HR 1.22, 95% CI 0.59-2.54); for ipsilateral non-perioperative stroke or TIA was 19.3% versus 17.2% (1.29, 0.78-2.14); and for any non-perioperative stroke was 21.1% versus 15.4% (1.66, 0.99-2.80).
Interpretation: More patients had stroke during follow-up in the endovascular group than in the surgical group, but the rate of ipsilateral non-perioperative stroke was low in both groups and none of the differences in the stroke outcome measures was significant. However, the study was underpowered and the confidence intervals were wide. More long-term data are needed from the on going stenting versus endarterectomy trials.
Funding: British Heart Foundation; UK National Health Service Management Executive; UK Stroke Association.
Figures
Comment in
-
Poor outcomes after endovascular treatment of symptomatic carotid stenosis: time for a moratorium.Lancet Neurol. 2009 Oct;8(10):871-3. doi: 10.1016/S1474-4422(09)70230-3. Epub 2009 Aug 28. Lancet Neurol. 2009. PMID: 19717346 No abstract available.
References
-
- European Carotid Surgery Trialists' Collaborative Group Randomised trial of endarterectomy for recently symptomatic carotid stenosis: final results of the MRC European Carotid Surgery Trial (ECST) Lancet. 1998;351:1379–1387. - PubMed
-
- Barnett HJ, Taylor DW, Eliasziw M. Benefit of carotid endarterectomy in patients with symptomatic moderate or severe stenosis. North American Symptomatic Carotid Endarterectomy Trial Collaborators. N Engl J Med. 1998;339:1415–1425. - PubMed
-
- Ederle J, Featherstone R, Brown M. Percutaneous transluminal angioplasty and stenting for carotid artery stenosis. Cochrane Database Syst Rev. 2007;4 CD000515. - PubMed
-
- Ederle J, Featherstone RL, Brown MM. Long-term outcome of endovascular treatment versus medical care for carotid artery stenosis in patients not suitable for surgery and randomised in the Carotid and Vertebral Artery Transluminal Angioplasty Study (CAVATAS) Cerebrovasc Dis. 2009;28:1–7. - PubMed
-
- Coward LJ, McCabe DJ, Ederle J, Featherstone RL, Clifton A, Brown MM. Long-term outcome after angioplasty and stenting for symptomatic vertebral artery stenosis compared with medical treatment in the Carotid And Vertebral Artery Transluminal Angioplasty Study (CAVATAS): a randomized trial. Stroke. 2007;38:1526–1530. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
