

Treatment of multiple myeloma: a comprehensive review
- PMID: 19717377
- PMCID: PMC3910142
- DOI: 10.3816/CLM.2009.n.056
Treatment of multiple myeloma: a comprehensive review
Abstract
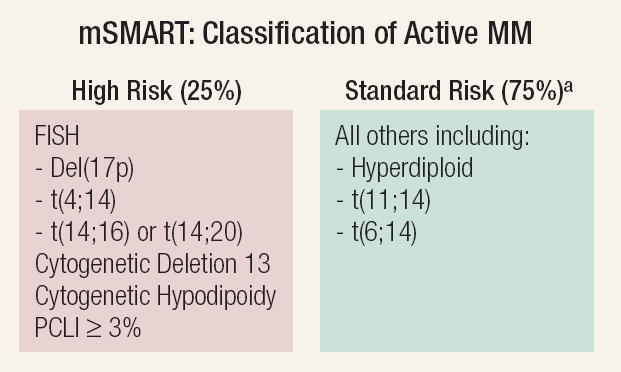
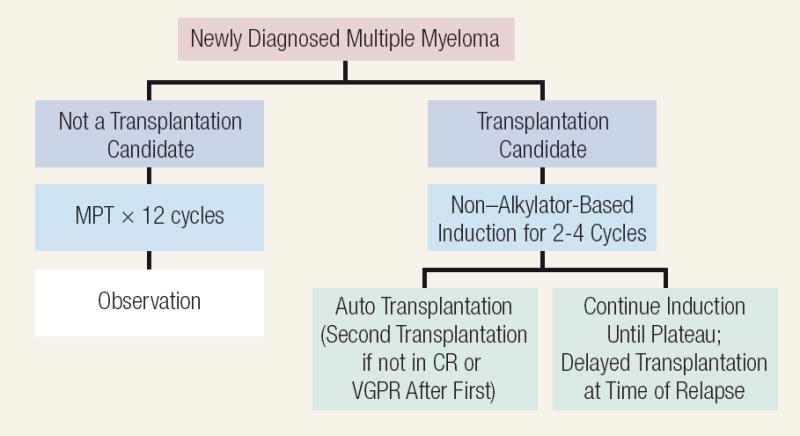
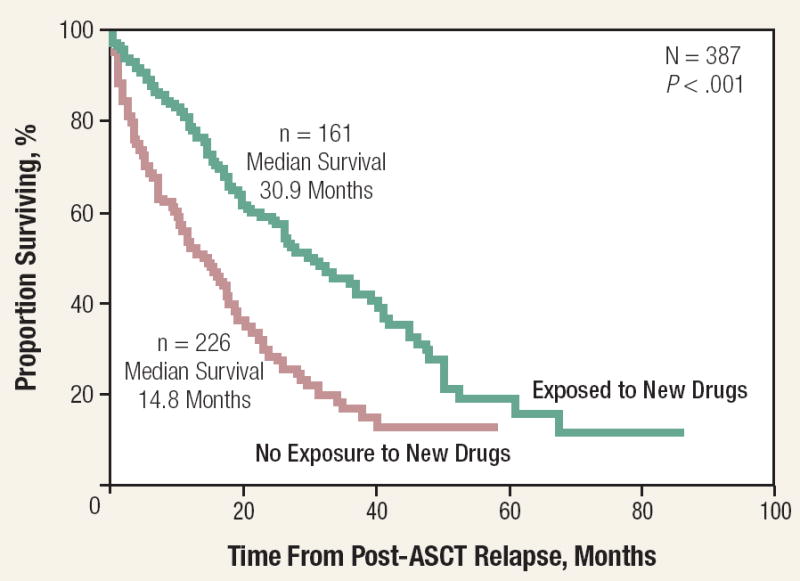
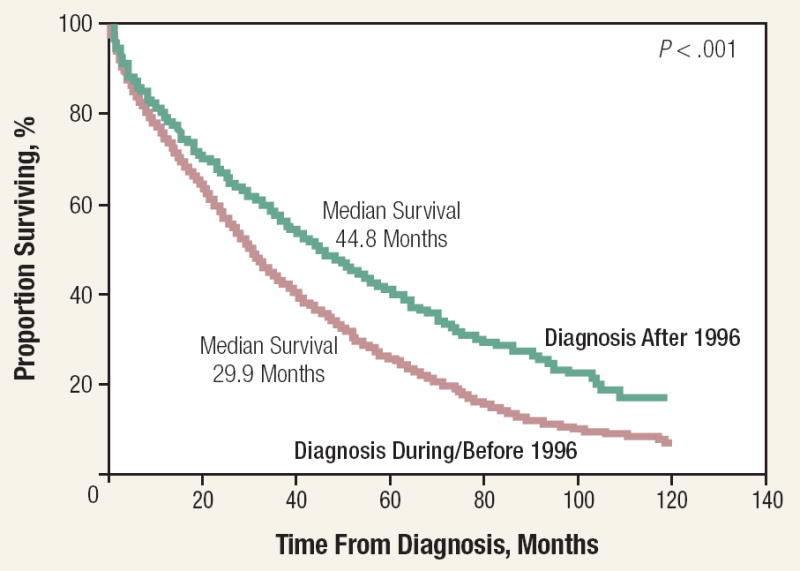
Multiple myeloma (MM) is a neoplastic plasma cell disorder that results in end-organ damage (hypercalcemia, renal insufficiency, anemia, or skeletal lesions). Patients should not be treated unless they have symptomatic (end-organ damage) MM. They should be classified as having high-risk or standard-risk disease. Patients are classified as high risk in the presence of hypodiploidy or deletion of chromosome 13 (del[13]) with conventional cytogenetics, the presence of t(4:14), t(14;16), t(14;20) translocations or del(17p) with fluorescence in situ hybridization. High-risk disease accounts for about 25% of patients with symptomatic MM. If the patient is deemed eligible for an autologous stem cell transplantation (ASCT), 3 or 4 cycles of lenalidomide and low-dose dexamethasone, or bortezomib and dexamethasone, or thalidomide and dexamethasone are reasonable choices. Stem cells should then be collected and one may proceed with an ASCT. If the patient has a complete response or a very good partial response (VGPR), the patient may be followed without maintenance therapy. If the patient has a less than VGPR, a second ASCT is encouraged. If the patient is in the high-risk group, a bortezomib-containing regimen to maximum response followed by 2 additional cycles of therapy is a reasonable approach. Lenalidomide and low-dose dexamethasone is another option for maintenance until progression. If the patient is considered ineligible for an ASCT, then melphalan, prednisone, and thalidomide is suggested for the standard-risk patient, and melphalan, prednisone, and bortezomib (MPV) for the high-risk patient. Treatment of relapsed or refractory MM is covered. The novel therapies-thalidomide, bortezomib, and lenalidomide-have resulted in improved survival rates. The complications of MM are also described. Multiple myeloma is a plasma cell neoplasm that is characterized by a single clone of plasma cells producing a monoclonal protein (M-protein). The malignant proliferation of plasma cells produces skeletal destruction that leads to bone pain and pathologic fractures. The M-protein might lead to renal failure, hyperviscosity syndrome, or through the suppression of uninvolved immunoglobulins, recurrent infections. Anemia and hypercalcemia are common complications.
Figures
References
-
- Kyle RA, Therneau TM, Rajkumar SV, et al. Incidence of multiple myeloma in Olmsted County, Minnesota - Trend over 6 decades. Cancer. 2004;101:2667–74. - PubMed
-
- Wingo PA, Ries LA, Rosenberg HM, et al. Cancer incidence and mortality, 1973-1995: a report card for the U.S. Cancer. 1998;82:1197–207. - PubMed
-
- Ries LA, et al., editors. SEER cancer statistics review, 1975-2003. Bethesda, MD: National Cancer Institute; 2006.
-
- Criteria for the classification of monoclonal gammopathies, multiple myeloma and related disorders: a report of the International Myeloma Working Group. Br J Haematol. 2003;121:749–57. - PubMed
-
- Rajkumar SV, Dispenzieri A, Kyle RA. Monoclonal gammopathy of undetermined significance, Waldenström macroglobulinemia, AL amyloidosis, and related plasma cell disorders: diagnosis and treatment. Mayo Clin Proc. 2006;81:693–703. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
