

Three-year follow-up and event rates in the international REduction of Atherothrombosis for Continued Health Registry
- PMID: 19720633
- PMCID: PMC2755116
- DOI: 10.1093/eurheartj/ehp355
Three-year follow-up and event rates in the international REduction of Atherothrombosis for Continued Health Registry
Abstract
Aims: To determine 3-year event rates in outpatients with vascular disease enrolled in the REduction of Atherothrombosis for Continued Health (REACH) Registry.
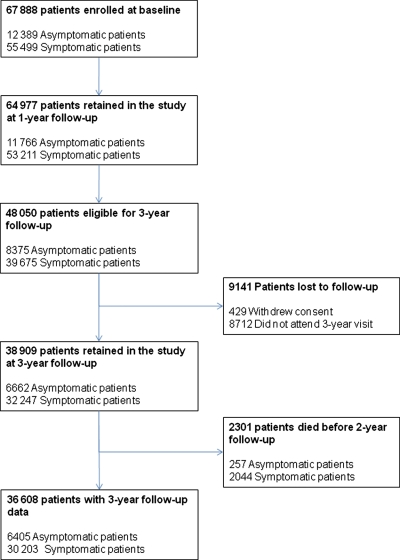
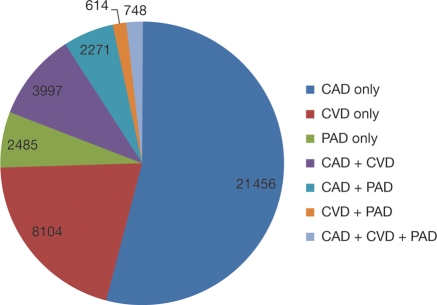
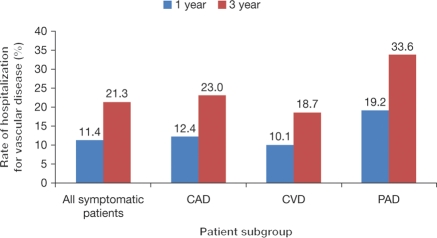
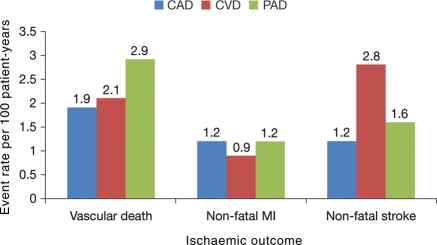
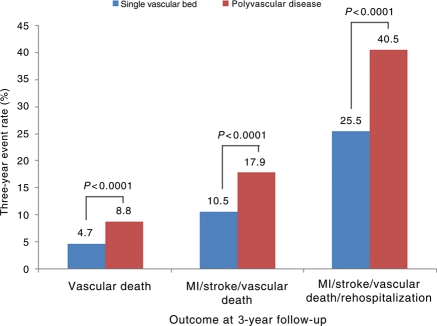
Methods and results: REACH enrolled 67 888 outpatients with atherothrombosis [established coronary artery disease (CAD), cerebrovascular disease, or peripheral arterial disease (PAD)], or with at least three atherothrombotic risk factors, from 44 countries. Among the 55 499 patients at baseline with symptomatic disease, 39 675 were eligible for 3-year follow-up, and 32 247 had data available (81% retention rate). Among the symptomatic patients at 3 years, 92% were taking an antithrombotic agent, 91% an antihypertensive, and 76% were on lipid-lowering therapy. For myocardial infarction (MI)/stroke/vascular death, 1- and 3-year event rates for all patients were 4.2 and 11.0%, respectively. Event rates (MI/stroke/vascular death) were significantly higher for patients with symptomatic disease vs. those with risk factors only at 1 year (4.7 vs. 2.3%, P < 0.001) and at 3 years (12.0 vs. 6.0%, P < 0.001). One and 3-year rates of MI/stroke/vascular death/rehospitalization were 14.4 and 28.4%, respectively, for patients with symptomatic disease. Rehospitalization for a vascular event other than MI/stroke/vascular death was common at 3 years (19.0% overall; 33.6% for PAD; 23.0% for CAD). For patients with symptomatic vascular disease in one vascular bed vs. multiple vascular beds, 3-year event rates for MI/stroke/vascular death/rehospitalization were 25.5 vs. 40.5% (P < 0.001).
Conclusion: Despite contemporary therapy, outpatients with symptomatic atherothrombotic vascular disease experience high rates of recurrent vascular events and rehospitalizations.
Figures
Comment in
-
Still a long way to go to defeating atherosclerotic disease: a call to arms!Eur Heart J. 2009 Oct;30(19):2297-9. doi: 10.1093/eurheartj/ehp356. Epub 2009 Aug 31. Eur Heart J. 2009. PMID: 19720634 No abstract available.
References
-
- Levenson JW, Skerrett PJ, Gaziano JM. Reducing the global burden of cardiovascular disease: the role of risk factors. Prev Cardiol. 2002;5:188–199. - PubMed
-
- Yusuf S, Reddy S, Ounpuu S, Anand S. Global burden of cardiovascular diseases: part I: general considerations, the epidemiologic transition, risk factors, and impact of urbanization. Circulation. 2001;104:2746–2753. - PubMed
-
- Dirks JH, Robinson SW, Alderman M, Couser WG, Grundy SM, Smith SC, Remuzzi G, Unwin N. Meeting report on the Bellagio Conference ‘prevention of vascular diseases in the emerging world: an approach to global health equity. Kidney Int. 2006;70:1397–1402. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
