

Unprotected left main revascularization in patients with acute coronary syndromes
- PMID: 19720640
- PMCID: PMC2755115
- DOI: 10.1093/eurheartj/ehp353
Unprotected left main revascularization in patients with acute coronary syndromes
Abstract
Aims: In acute coronary syndromes (ACS), the optimal revascularization strategy for unprotected left main coronary disease (ULMCD) has been little studied. The objectives of the present study were to describe the practice of ULMCD revascularization in ACS patients and its evolution over an 8-year period, analyse the prognosis of this population and determine the effect of revascularization on outcome.
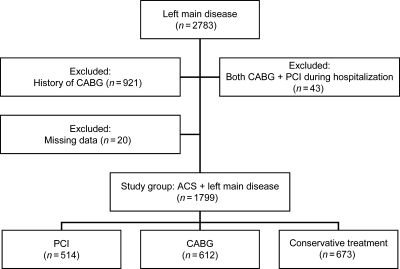
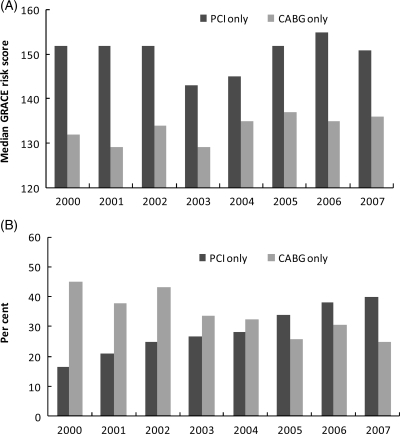
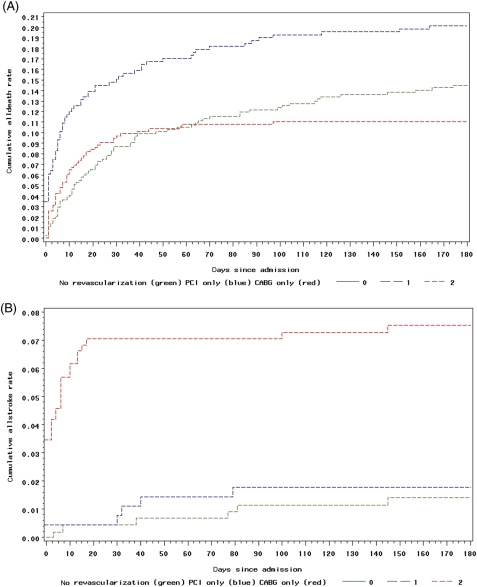
Methods and results: Of 43 018 patients enrolled in the Global Registry of Acute Coronary Events (GRACE) between 2000 and 2007, 1799 had significant ULMCD and underwent percutaneous coronary intervention (PCI) alone (n = 514), coronary artery bypass graft (CABG) alone (n = 612), or no revascularization (n = 673). Mortality was 7.7% in hospital and 14% at 6 months. Over the 8-year study, the GRACE risk score remained constant, but there was a steady shift to more PCI than CABG over time. Patients undergoing PCI presented more frequently with ST-segment elevation myocardial infarction (STEMI), after cardiac arrest, or in cardiogenic shock; 48% of PCI patients underwent revascularization on the day of admission vs. 5.1% in the CABG group. After adjustment, revascularization was associated with an early hazard of hospital death vs. no revascularization, significant for PCI (hazard ratio (HR) 2.60, 95% confidence interval (CI) 1.62-4.18) but not for CABG (1.26, 0.72-2.22). From discharge to 6 months, both PCI (HR 0.45, 95% CI 0.23-0.85) and CABG (0.11, 0.04-0.28) were significantly associated with improved survival in comparison with an initial strategy of no revascularization. Coronary artery bypass graft revascularization was associated with a five-fold increase in stroke compared with the other two groups.
Conclusion: Unprotected left main coronary disease in ACS is associated with high mortality, especially in patients with STEMI and/or haemodynamic or arrhythmic instability. Percutaneous coronary intervention is now the most common revascularization strategy and preferred in higher risk patients. Coronary artery bypass graft is often delayed and performed in lower risk patients, leading to good 6-month survival. The two approaches therefore appear complementary.
Figures
Comment in
-
PCI in acute left main disease: a paradigm shift or a new reality?Eur Heart J. 2009 Oct;30(19):2295-6. doi: 10.1093/eurheartj/ehp354. Epub 2009 Aug 30. Eur Heart J. 2009. PMID: 19720641 No abstract available.
References
-
- Varnauskas E. Twelve-year follow-up of survival in the randomized European Coronary Surgery Study. N Engl J Med. 1988;319:332–337. - PubMed
-
- Chaitman BR, Fisher LD, Bourassa MG, Davis K, Rogers WJ, Maynard C, Tyras DH, Berger RL, Judkins MP, Ringqvist I, Mock MB, Killip T. Effect of coronary bypass surgery on survival patterns in subsets of patients with left main coronary artery disease. Report of the Collaborative Study in Coronary Artery Surgery (CASS) Am J Cardiol. 1981;48:765–777. - PubMed
-
- Park SJ, Park SW, Hong MK, Cheong SS, Lee CW, Kim JJ, Hong MK, Mintz GS, Leon MB. Stenting of unprotected left main coronary artery stenoses: immediate and late outcomes. J Am Coll Cardiol. 1998;31:37–42. - PubMed
-
- Black A, Cortina R, Bossi I, Choussat R, Fajadet J, Marco J. Unprotected left main coronary artery stenting: correlates of mid-term survival and impact of patient selection. J Am Coll Cardiol. 2001;37:832–838. - PubMed
-
- Silvestri M, Barragan P, Sainsous J, Bayet G, Simeoni JB, Roquebert PO, Macaluso G, Bouvier JL, Comet B. Unprotected left main coronary artery stenting: immediate and medium-term outcomes of 140 elective procedures. J Am Coll Cardiol. 2000;35:1543–1550. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
