

Impact of the PPAR-gamma2 Pro12Ala polymorphism and ACE inhibitor therapy on new-onset microalbuminuria in type 2 diabetes: evidence from BENEDICT
- PMID: 19720797
- PMCID: PMC2780880
- DOI: 10.2337/db09-0407
Impact of the PPAR-gamma2 Pro12Ala polymorphism and ACE inhibitor therapy on new-onset microalbuminuria in type 2 diabetes: evidence from BENEDICT
Abstract
Objective: Cross-sectional studies found less microalbuminuria in type 2 diabetic patients with the Ala12 allele of the peroxisome proliferator-activated receptor-gamma2 (PPAR-gamma2) Pro12Ala polymorphism. We prospectively evaluated the association between Pro12Ala polymorphism (rs1801282) and new-onset microalbuminuria.
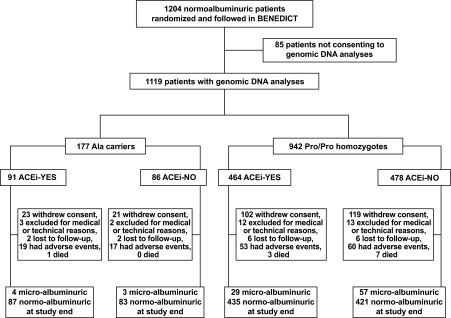
Research design and methods: Pro12Ala polymorphism was genotyped by TaqMan-based assay in genomic DNA of 1,119 consenting patients from BErgamo NEphrologic DIabetic Complications Trial (BENEDICT)-a prospective, randomized trial evaluating ACE inhibition effect on new-onset microalbuminuria (albuminuria 20-200 microg/min in at least two of three consecutive overnight urine collections in two consecutive visits) in hypertensive type 2 diabetes with albuminuria <20 microg/min at inclusion.
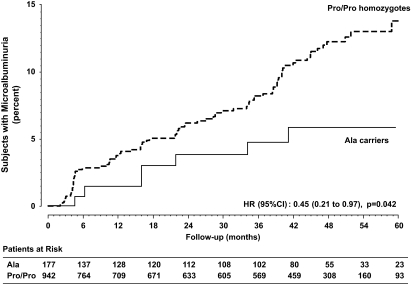
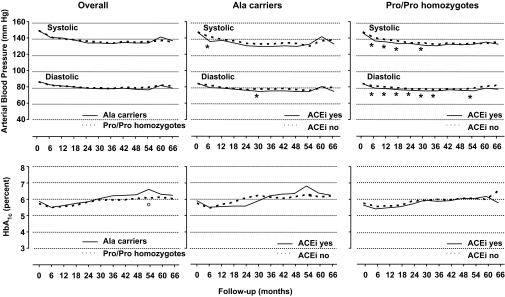
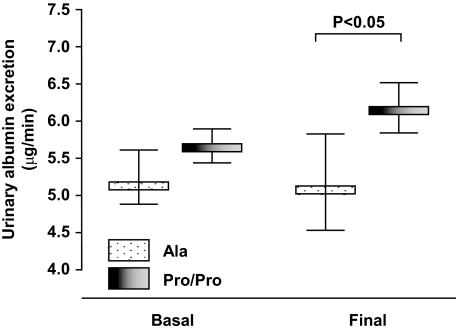
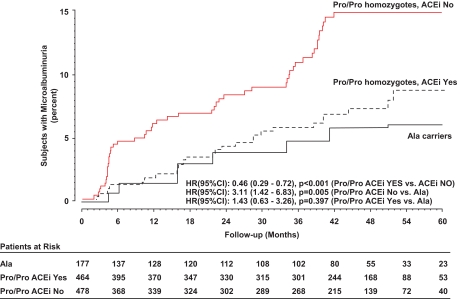
Results: Baseline characteristics of Ala (Ala/Ala or Ala/Pro) carriers and Pro/Pro homozygotes were similar, with a nonsignificant trend to lower albuminuria (P = 0.1107) in the 177 Ala carriers. Over a median (interquartile range) of 44.0 (17.1-51.9) months, 7 (4%) Ala carriers and 86 (9.1%) Pro/Pro homozygotes developed microalbuminuria (hazard ratio [HR] 0.45 [95% CI 0.21-0.97]; P = 0.042). Final albuminuria was significantly lower in Ala carriers than Pro/Pro homozygotes (7.3 +/- 9.1 vs. 10.5 +/- 24.9 microg/min, respectively), even after adjustment for baseline albuminuria (P = 0.048). Baseline and follow-up blood pressure and metabolic control were similar in both groups. Incidence of microalbuminuria was significantly decreased by ACE versus non-ACE inhibitor therapy in Pro/Pro homozygotes (6.3 vs. 11.9%, respectively, HR 0.46 [0.29-0.72]; P < 0.001).
Conclusions: In type 2 diabetes, the Ala allele protects from worsening albuminuria and new-onset microalbuminuria, and ACE inhibition blunts the excess risk of microalbuminuria associated with the Pro/Pro genotype. Evaluating Pro12Ala polymorphism may help identifying patients at risk who may benefit the most from early renoprotective therapy.
Figures
References
-
- Viberti GC, Hill RD, Jarrett RJ, Argyropoulos A, Mahmud U, Keen H: Microalbuminuria as a predictor of clinical nephropathy in insulin-dependent diabetes mellitus. Lancet 1982; 1: 1430– 1432 - PubMed
-
- Borch-Johnsen K, Feldt-Rasmussen B, Strandgaard S, Schroll M, Jensen JS: Urinary albumin excretion: an independent predictor of ischemic heart disease. Arterioscler Thromb Vasc Biol 1999; 19: 1992– 1997 - PubMed
-
- Hillege HL, Fidler V, Diercks GF, van Gilst WH, de Zeeuw D, van Veldhuisen DJ, Gans RO, Janssen WM, Grobbee DE, de Jong PE: Urinary albumin excretion predicts cardiovascular and noncardiovascular mortality in general population. Circulation 2002; 106: 1777– 1782 - PubMed
-
- Klausen K, Borch-Johnsen K, Feldt-Rasmussen B, Jensen G, Clausen P, Scharling H, Appleyard M, Jensen JS: Very low levels of microalbuminuria are associated with increased risk of coronary heart disease and death independently of renal function, hypertension, and diabetes. Circulation 2004; 110: 32– 35 - PubMed
-
- Arnlov J, Evans JC, Meigs JB, Wang TJ, Fox CS, Levy D, Benjamin EJ, D'Agostino RB, Vasan RS: Low-grade albuminuria and incidence of cardiovascular disease events in nonhypertensive and nondiabetic individuals: the Framingham Heart Study. Circulation 2005; 112: 969– 975 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
