

Phase II, randomized, placebo-controlled trial of neoadjuvant celecoxib in men with clinically localized prostate cancer: evaluation of drug-specific biomarkers
- PMID: 19720908
- PMCID: PMC2799055
- DOI: 10.1200/JCO.2009.21.9410
Phase II, randomized, placebo-controlled trial of neoadjuvant celecoxib in men with clinically localized prostate cancer: evaluation of drug-specific biomarkers
Abstract
Purpose: Cyclooxygenase-2 (COX-2) is a potential pharmacologic target for the prevention of various malignancies, including prostate cancer. We conducted a randomized, double-blind trial to examine the effect of celecoxib on drug-specific biomarkers from prostate tissue obtained at prostatectomy.
Patients and methods: Patients with localized prostate cancer and Gleason sum > or = 7, prostate-specific antigen (PSA) > or = 15 ng/mL, clinical stage T2b or greater, or any combination with greater than 45% risk of capsular penetration were randomly assigned to celecoxib 400 mg by mouth twice daily or placebo for 4 to 6 weeks before prostatectomy. The primary end point was the difference in prostatic prostaglandin levels between the two groups. Secondary end points were differences in COX-1 and -2 expressions; oxidized DNA bases; and markers of proliferation, apoptosis and angiogenesis. Tissue celecoxib concentrations also were measured. Tertiary end points were drug safety and compliance.
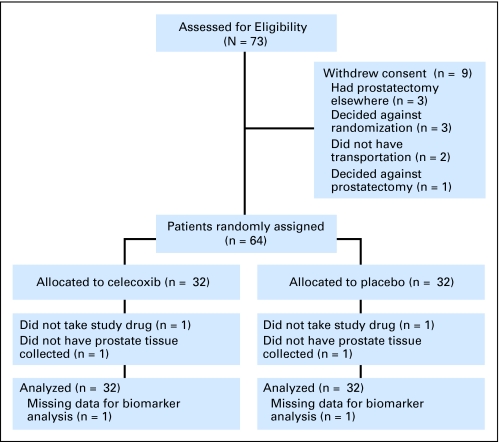
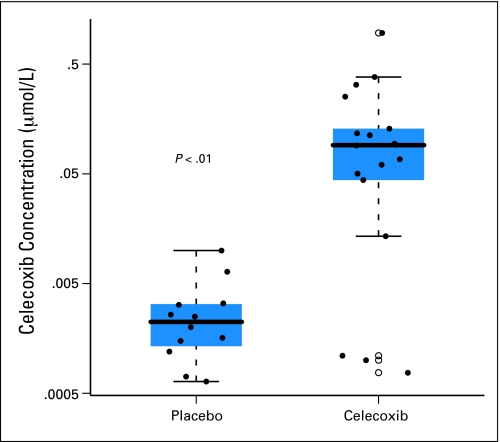
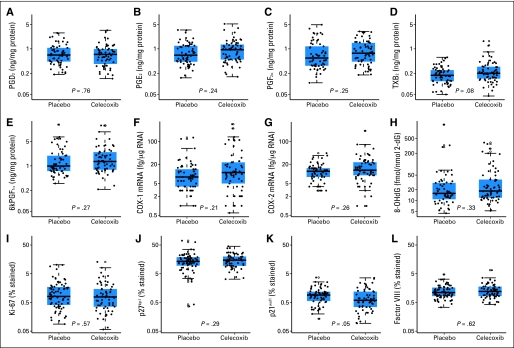
Results: Seventy-three patients consented, and 64 were randomly assigned and included in the intention-to-treat analysis. There were no treatment differences in any of the primary or secondary outcomes. Multivariable regression revealed that tumor tissue had significantly lower COX-2 expression than benign prostatic tissue (P = .01) and significantly higher levels of the proliferation marker Ki-67 (P < .0001). Celecoxib was measurable in prostate tissue of patients on treatment, demonstrating that celecoxib reached its target. Celecoxib was safe and resulted in only grade 1 toxicities.
Conclusion: Treatment with 4 to 6 weeks of celecoxib had no effect on intermediate biomarkers of prostate carcinogenesis, despite the achievement of measurable tissue levels. We caution against using celecoxib 400 mg twice daily as a preventive agent for prostate cancer in additional studies.
Conflict of interest statement
Authors' disclosures of potential conflicts of interest and author contributions are found at the end of this article.
Figures
Comment in
-
Informative clinical investigation: a demanding taskmaster.J Clin Oncol. 2009 Oct 20;27(30):4937-8. doi: 10.1200/JCO.2009.23.8063. Epub 2009 Aug 31. J Clin Oncol. 2009. PMID: 19720892 No abstract available.
References
-
- Jemal A, Siegel R, Ward E, et al. Cancer statistics, 2008. CA Cancer J Clin. 2008;58:71–96. - PubMed
-
- Nelson WG, De Marzo AM, Isaacs WB. Prostate cancer. N Engl J Med. 2003;349:366–381. - PubMed
-
- Putzi MJ, De Marzo AM. Morphologic transitions between proliferative inflammatory atrophy and high-grade prostatic intraepithelial neoplasia. Urology. 2000;56:828–832. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
