

Centralization of cancer surgery: implications for patient access to optimal care
- PMID: 19720926
- PMCID: PMC3039919
- DOI: 10.1200/JCO.2008.20.1715
Centralization of cancer surgery: implications for patient access to optimal care
Abstract
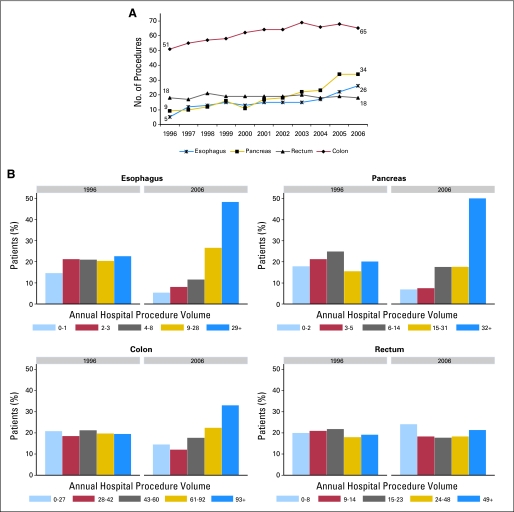
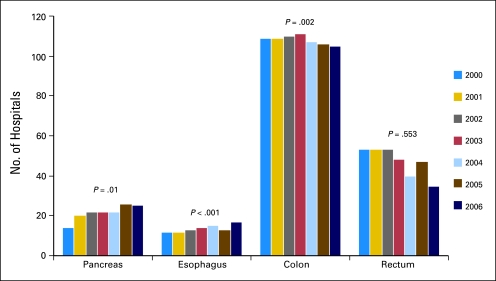
Purpose: The volume-outcomes relationship has led many to advocate centralization of cancer procedures at high volume hospitals (HVH). We hypothesized that in response cancer surgery has become increasingly centralized and that this centralization has resulted in increased travel burden for patients.
Patients and methods: Using 1996 to 2006 discharge data from NY, NJ, PA, all patients > or = 18 years old treated with extirpative surgery for colorectal, esophageal, or pancreatic cancer were examined. Patients and hospitals were geocoded. Annual hospital procedure volume for each tumor site was examined, and multiple quantile and logistic regressions were used to compare changes in centralization and distance traveled.
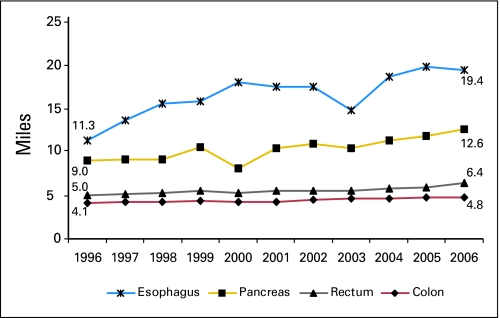
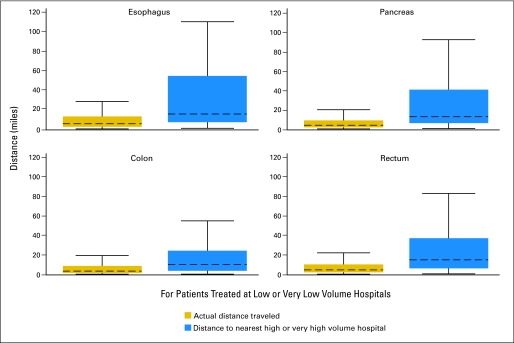
Results: Five thousand two hundred seventy-three esophageal, 13,472 pancreatic, 202,879 colon, and 51,262 rectal procedures were included. A shift to HVH occurred to varying degrees for all tumor types. The odds of surgery at a low volume hospital decreased for esophagus, pancreas and colon: per year odds ratios (ORs) were 0.87 (95% CI, 0.85 to 0.90), 0.85 (95% CI, 0.84 to 0.87), and 0.97 (95% CI, 0.97 to 0.98). Median travel distance increased for all sites: esophagus 72%, pancreas 40%, colon 17%, and rectum 28% (P < .0001). Travel distance was proportional to procedure volume (P < .0001). The majority of the increase in distance was attributable to centralization.
Conclusion: There has been extensive centralization of complex cancer surgery over the past decade. While this process should result in population-level improvements in cancer outcomes, centralization is increasing patient travel. For some subsets of the population, increasing travel requirements may pose a significant barrier to access to quality cancer care.
Conflict of interest statement
Authors' disclosures of potential conflicts of interest and author contributions are found at the end of this article.
Figures
Comment in
-
Centralization of cancer surgery: what does it mean for surgical training?J Clin Oncol. 2009 Oct 1;27(28):4637-9. doi: 10.1200/JCO.2009.23.0052. Epub 2009 Aug 31. J Clin Oncol. 2009. PMID: 19720900 No abstract available.
References
-
- Luft HS, Bunker JP, Enthoven AC. Should operations be regionalized? The empirical relation between surgical volume and mortality. N Engl J Med. 1979;301:1364–1369. - PubMed
-
- Birkmeyer JD, Siewers AE, Finlayson EV, et al. Hospital volume and surgical mortality in the United States. N Engl J Med. 2002;346:1128–1137. - PubMed
-
- Begg CB, Cramer LD, Hoskins WJ, et al. Impact of hospital volume on operative mortality for major cancer surgery. JAMA. 1998;280:1747–1751. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
