

The net clinical benefit of warfarin anticoagulation in atrial fibrillation
- PMID: 19721017
- PMCID: PMC2777526
- DOI: 10.7326/0003-4819-151-5-200909010-00003
The net clinical benefit of warfarin anticoagulation in atrial fibrillation
Abstract
Background: Guidelines recommend warfarin use in patients with atrial fibrillation solely on the basis of risk for ischemic stroke without antithrombotic therapy. These guidelines rely on ischemic stroke rates observed in older trials and do not explicitly account for increased risk for hemorrhage.
Objective: To quantify the net clinical benefit of warfarin therapy in a cohort of patients with atrial fibrillation.
Design: Mixed retrospective and prospective cohort study of patients with atrial fibrillation between 1996 and 2003.
Setting: An integrated health care delivery system.
Patients: 13 559 adults with nonvalvular atrial fibrillation.
Measurements: Warfarin exposure, patient characteristics, CHADS(2) score (1 point for each of congestive heart failure, hypertension, age, and diabetes and 2 points for stroke), and outcome events were ascertained from health plan records and databases. Net clinical benefit was defined as the annual rate of ischemic strokes and systemic emboli prevented by warfarin minus intracranial hemorrhages attributable to warfarin, multiplied by an impact weight. The base-case impact weight was 1.5, reflecting the greater clinical impact of intracranial hemorrhage versus thromboembolism.
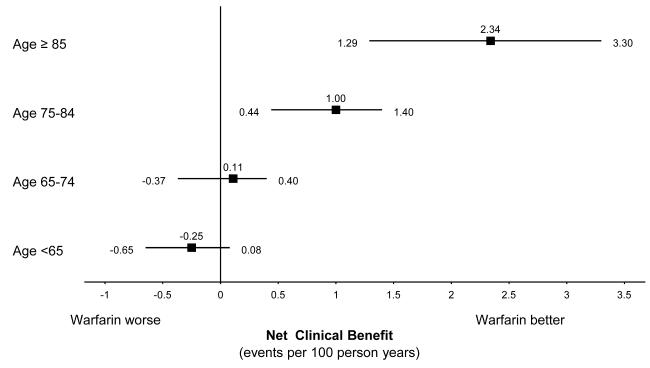
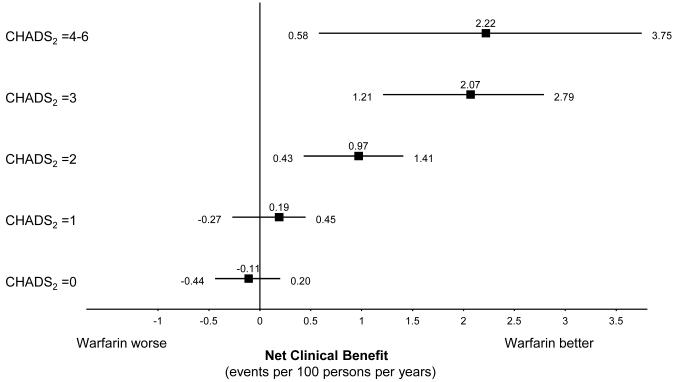
Results: Patients accumulated more than 66 000 person-years of follow-up. The adjusted net clinical benefit of warfarin for the cohort overall was 0.68% per year (95% CI, 0.34% to 0.87%). Adjusted net clinical benefit was greatest for patients with a history of ischemic stroke (2.48% per year [CI, 0.75% to 4.22%]) and for those 85 years or older (2.34% per year [CI, 1.29% to 3.30%]). The net clinical benefit of warfarin increased from essentially zero in CHADS(2) stroke risk categories 0 and 1 to 2.22% per year (CI, 0.58% to 3.75%) in CHADS(2) categories 4 to 6. The patterns of results were preserved when weighting factors for intracranial hemorrhage of 1.0 and 2.0 were used.
Limitations: Residual confounding is a possibility. Some outcome events were probably missed by the screening algorithm or when medical records were unavailable.
Conclusion: Expected net clinical benefit of warfarin therapy is highest among patients with the highest untreated risk for stroke, which includes the oldest age category. Risk assessment that incorporates both risk for thromboembolism and risk for intracranial hemorrhage provides a more quantitatively informed basis for the decision on antithrombotic therapy in patients with atrial fibrillation.
Primary funding source: National Institute on Aging; National Heart, Lung, and Blood Institute; and Massachusetts General Hospital.
Figures
Comment in
-
Do current guidelines result in overuse of warfarin anticoagulation in patients with atrial fibrillation?Ann Intern Med. 2009 Sep 1;151(5):355-6. doi: 10.7326/0003-4819-151-5-200909010-00012. Ann Intern Med. 2009. PMID: 19721024 No abstract available.
-
The net clinical benefit of warfarin anticoagulation in atrial fibrillation.Ann Intern Med. 2010 Feb 16;152(4):264-5; author reply 265. doi: 10.7326/0003-4819-152-4-201002160-00016. Ann Intern Med. 2010. PMID: 20157144 No abstract available.
-
The net clinical benefit of warfarin anticoagulation in atrial fibrillation.Ann Intern Med. 2010 Feb 16;152(4):265. doi: 10.7326/0003-4819-152-4-201002160-00017. Ann Intern Med. 2010. PMID: 20157146 No abstract available.
Summary for patients in
-
Summaries for patients. Net benefit of warfarin in atrial fibrillation.Ann Intern Med. 2009 Sep 1;151(5):I36. doi: 10.7326/0003-4819-151-5-200909010-00001. Ann Intern Med. 2009. PMID: 19721014 No abstract available.
References
-
- Gage BF, Waterman AD, Shannon W, Boechler M, Rich MW, Radford MJ. Validation of clinical classification schemes for predicting stroke: results from the National Registry of Atrial Fibrillation. JAMA. 2001 Jun 13;285(22):2864–2870. - PubMed
-
- Risk factors for stroke and efficacy of antithrombotic therapy in atrial fibrillation. Analysis of pooled data from five randomized controlled trials. Arch Intern Med. 1994;154:1449–57. [PMID: 8018000] - PubMed
-
- Go AS, Hylek EM, Chang Y, Phillips KA, Henault LE, Capra AM, et al. Anticoagulation therapy for stroke prevention in atrial fibrillation: how well do randomized trials translate into clinical practice? JAMA. 2003;290:2685–92. [PMID: 14645310] - PubMed
-
- Fuster V, Rydén LE, Cannom DS, Crijns HJ, Curtis AB, Ellenbogen KA, et al. American College of Cardiology ACC/AHA/ESC 2006 guidelines for the management of patients with atrial fibrillation: full text: a report of the American College of Cardiology/American Heart Association Task Force on practice guidelines and the European Society of Cardiology Committee for Practice Guidelines (Writing Committee to Revise the 2001 guidelines for the management of patients with atrial fibrillation) developed in collaboration with the European Heart Rhythm Association and the Heart Rhythm Society. Europace. 2006;8:651–745. [PMID: 16987906] - PubMed
-
- Singer DE, Albers GW, Dalen JE, Fang MC, Go AS, Halperin JL, et al. American College of Chest Physicians Antithrombotic therapy in atrial fibrillation: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines (8th Edition) Chest. 2008;133:546S–592S. [PMID: 18574273] - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical