

The impact of the demographic transition on dengue in Thailand: insights from a statistical analysis and mathematical modeling
- PMID: 19721696
- PMCID: PMC2726436
- DOI: 10.1371/journal.pmed.1000139
The impact of the demographic transition on dengue in Thailand: insights from a statistical analysis and mathematical modeling
Abstract
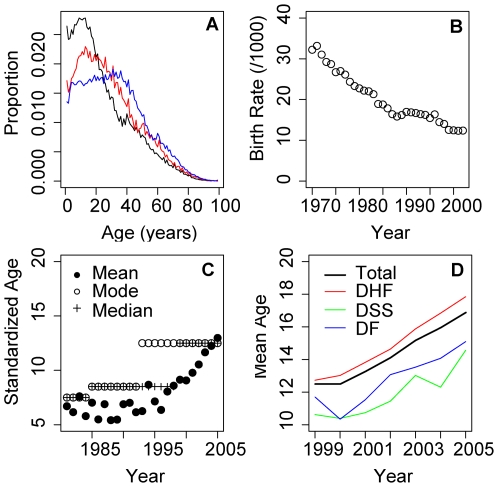
Background: An increase in the average age of dengue hemorrhagic fever (DHF) cases has been reported in Thailand. The cause of this increase is not known. Possible explanations include a reduction in transmission due to declining mosquito populations, declining contact between human and mosquito, and changes in reporting. We propose that a demographic shift toward lower birth and death rates has reduced dengue transmission and lengthened the interval between large epidemics.
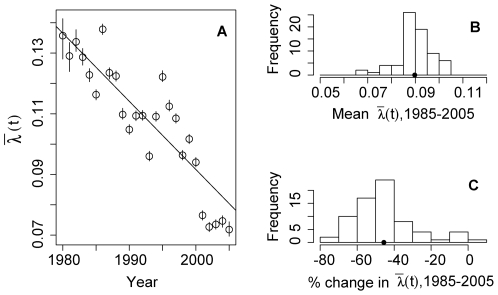
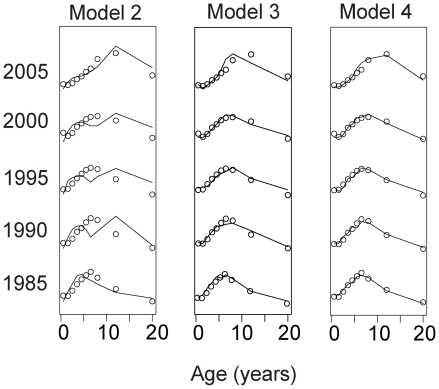
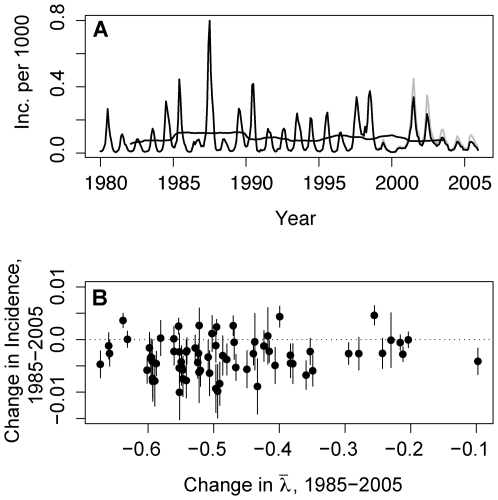
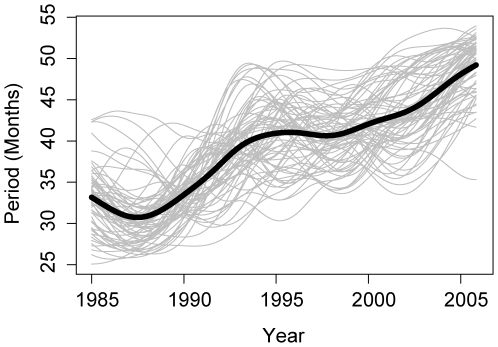
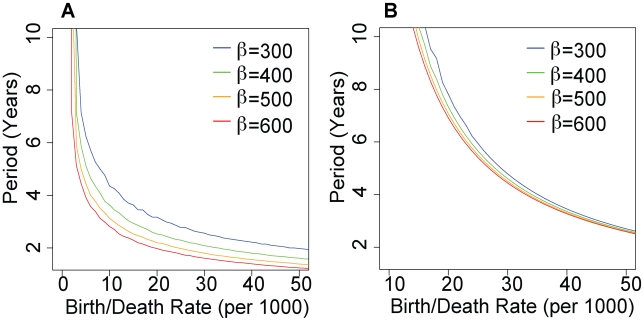
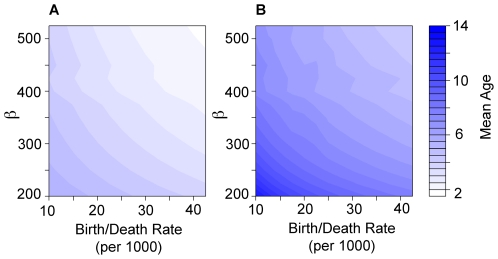
Methods and findings: Using data from each of the 72 provinces of Thailand, we looked for associations between force of infection (a measure of hazard, defined as the rate per capita at which susceptible individuals become infected) and demographic and climactic variables. We estimated the force of infection from the age distribution of cases from 1985 to 2005. We find that the force of infection has declined by 2% each year since a peak in the late 1970s and early 1980s. Contrary to recent findings suggesting that the incidence of DHF has increased in Thailand, we find a small but statistically significant decline in DHF incidence since 1985 in a majority of provinces. The strongest predictor of the change in force of infection and the mean force of infection is the median age of the population. Using mathematical simulations of dengue transmission we show that a reduced birth rate and a shift in the population's age structure can explain the shift in the age distribution of cases, reduction of the force of infection, and increase in the periodicity of multiannual oscillations of DHF incidence in the absence of other changes.
Conclusions: Lower birth and death rates decrease the flow of susceptible individuals into the population and increase the longevity of immune individuals. The increase in the proportion of the population that is immune increases the likelihood that an infectious mosquito will feed on an immune individual, reducing the force of infection. Though the force of infection has decreased by half, we find that the critical vaccination fraction has not changed significantly, declining from an average of 85% to 80%. Clinical guidelines should consider the impact of continued increases in the age of dengue cases in Thailand. Countries in the region lagging behind Thailand in the demographic transition may experience the same increase as their population ages. The impact of demographic changes on the force of infection has been hypothesized for other diseases, but, to our knowledge, this is the first observation of this phenomenon. Please see later in the article for the Editors' Summary.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Comment in
-
Changing patterns of dengue epidemiology and implications for clinical management and vaccines.PLoS Med. 2009 Sep;6(9):e1000129. doi: 10.1371/journal.pmed.1000129. Epub 2009 Sep 1. PLoS Med. 2009. PMID: 19721698 Free PMC article.
References
-
- Kongsomboon K, Singhasivanon P, Kaewkungwal J, Nimmannitya S, Mammen MP, Jr, et al. Temporal trends of dengue fever/dengue hemorrhagic fever in Bangkok, Thailand from 1981 to 2000: an age-period-cohort analysis. Southeast Asian J Trop Med Public Health. 2004;35:913–917. - PubMed
-
- Malavige GN, Velathanthiri VG, Wijewickrama ES, Fernando S, Jayaratne SD, et al. Patterns of disease among adults hospitalized with dengue infections. QJM. 2006;99:299–305. - PubMed
-
- Thai KT, Binh TQ, Giao PT, Phuong HL, Hung lQ, et al. Seroprevalence of dengue antibodies, annual incidence and risk factors among children in southern Vietnam. Trop Med Int Health. 2005;10:379–386. - PubMed
-
- Wichmann O, Hongsiriwon S, Bowonwatanuwong C, Chotivanich K, Sukthana Y, et al. Risk factors and clinical features associated with severe dengue infection in adults and children during the 2001 epidemic in Chonburi, Thailand. Trop Med Int Health. 2004;9:1022–1029. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
