

Imaging findings of rhinocerebral mucormycosis
- PMID: 19721767
- PMCID: PMC2671302
- DOI: 10.1055/s-0028-1096209
Imaging findings of rhinocerebral mucormycosis
Abstract
Background and objectives: The purpose of this study was to describe common radiographic patterns that may be useful in predicting the diagnosis of rhinocerebral mucormycosis.
Methods: We retrospectively evaluated the imaging and clinical data of four males and one female, 3 to 72 years old, with rhinocerebral mucormycosis.
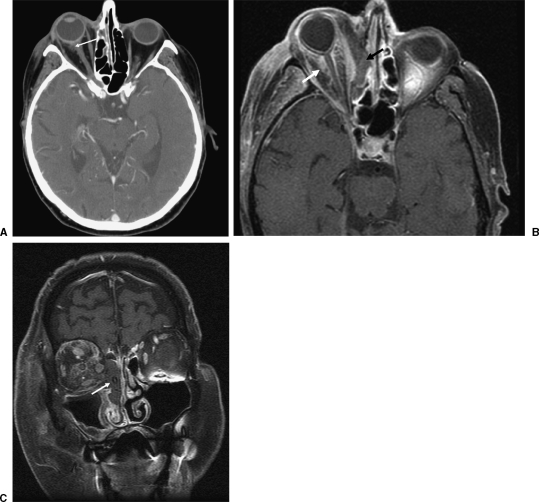
Results: All the patients presented with sinusitis and ophthalmological symptoms. Most of the patients (80%) had isointense lesions relative to brain in T1-weighted images. The signal intensity in T2-weighted images was more variable, with only one (20%) patient showing hyperintensity. A pattern of anatomic involvement affecting the nasal cavity, maxillary sinus, orbit, and ethmoid cells was consistently observed in all five patients (100%). Our series demonstrated a mortality rate of 60%.
Conclusion: Progressive and rapid involvement of the cavernous sinus, vascular structures and intracranial contents is the usual evolution of rhinocerebral mucormycosis. In the context of immunosupression, a pattern of nasal cavity, maxillary sinus, ethmoid cells, and orbit inflammatory lesions should prompt the diagnosis of mucormycosis. Multiplanar magnetic resonance imaging shows anatomic involvement, helping in surgery planning. However, the prognosis is grave despite radical surgery and antifungals.
Keywords: MRI; Rhinocerebral mucormycosis; imaging findings; neuroradiology.
Figures







References
-
- Anselmo-Lima W T, Lopes R P, Valera F C, et al. Invasive fungal rhinosinusitis in immunocompromised patients. Rhinology. 2004;42:141–144. - PubMed
-
- Paulltauf A. Mycosis mucorina. Virchows Arch. 1885;102:543.
-
- Naussbaum E S, Holl W A. Rhinocerebral mucormycosis: changing patterns of disease. Surg Neurol. 1994;41:152–156. - PubMed
