

Review
doi: 10.3348/kjr.2009.10.5.496.
Epub 2009 Aug 25.
Radiation-induced complications after breast cancer radiation therapy: a pictorial review of multimodality imaging findings
Affiliations
- PMID: 19721835
- PMCID: PMC2731868
- DOI: 10.3348/kjr.2009.10.5.496
Item in Clipboard
Review
Radiation-induced complications after breast cancer radiation therapy: a pictorial review of multimodality imaging findings
Korean J Radiol.
2009 Sep-Oct.
Abstract
The purpose of this pictorial essay is to illustrate the multimodality imaging findings of a wide spectrum of radiation-induced complications of breast cancer in the sequence of occurrence. We have classified radiation-induced complications into three groups based on the time sequence of occurrence. Knowledge of these findings will allow for the early detection of complications as well as the ability to differentiate tumor recurrence.
Keywords: Breast, neoplasms; Radiation therapy, CT; Radiation therapy, MRI; Radiation therapy, PET; Radiation therapy, US.
Figures
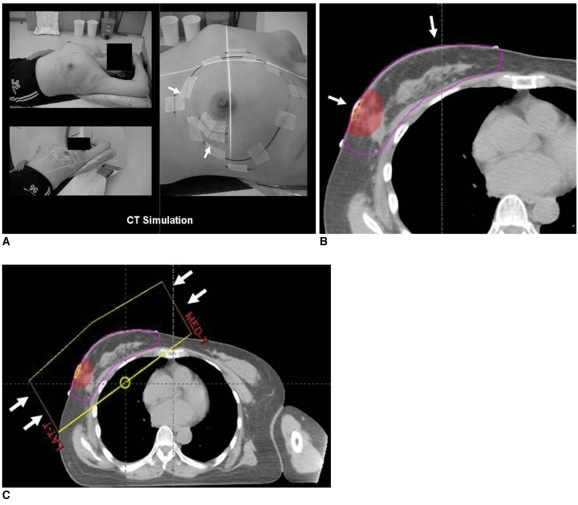
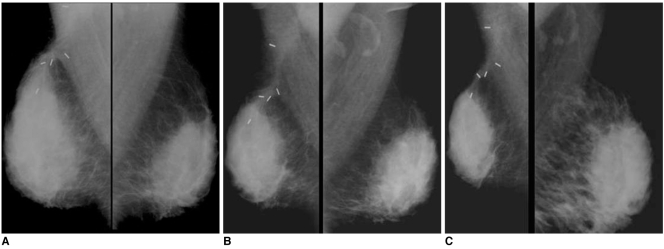
External beam radiation is usual type of radiation therapy for breast cancer. Three steps of external beam radiation include (A) CT simulation (arrows), (B) contouring of targeted site (arrows) and (C) tangential two-field planning (arrows).
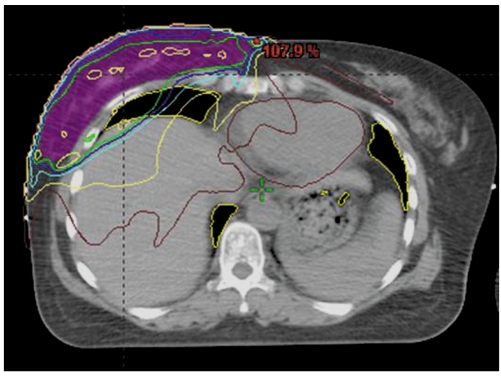
Radiation affects adjacent structures as well as operation bed with entire breast including following: target breast, overlying skin, chest wall, lung, heart, opposite breast and adjacent organs.
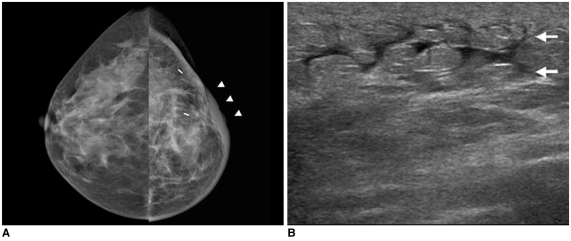
42-year-old female patient who had undergone radiation therapy in left breast six months ago are shown. A. Mammography of left breast shows diffuse skin and trabecular thickening (arrowheads). B. US of left breast shows diffuse skin thickening and interstitial edema (arrows).
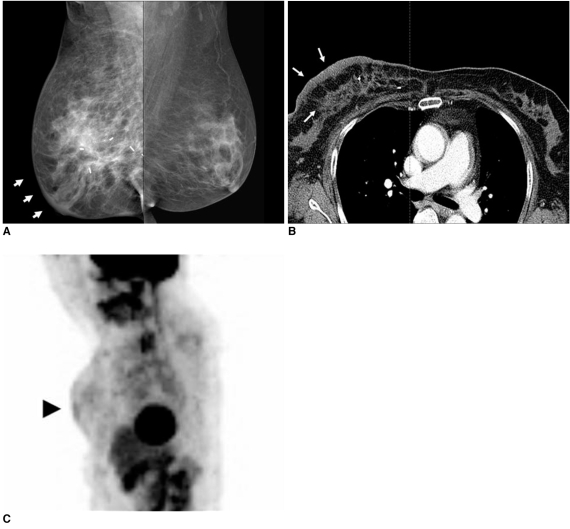
53-year-old female patient who had undergone radiation therapy in right breast six months ago are shown. A. Mammography of right breast shows diffusely increased density due to skin and trabecular thickening (arrows). B. Chest CT scan shows diffuse breast edema with skin and trabecular thickening (arrows). C. Whole body PET image shows diffuse skin thickening and interstitial edema with mild hypermetabolic activity (max SUV = 1.8) (arrowhead) in irradiated right breast.
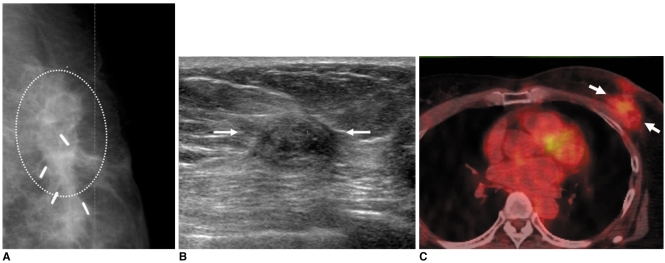
55-year-old female patient with hard palpable mass who had undergone radiation therapy in left breast two years ago are shown. A. Mammography shows mass with spiculated margin, irregular shape and internal fat density (circle). B. US study of left breast shows presence of isoechoic mass with spiculated margin and irregular shape (arrows). C. Whole body PET/CT image shows mass with hypermetabolic activity (max SUV = 2.4) (arrows). Patient was diagnosed as having radiation-induced fat necrosis.
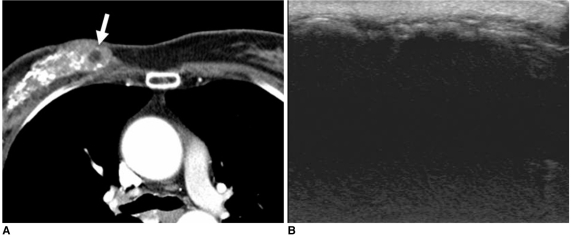
45-year-old female patient who had undergone radiation therapy in right breast one year ago are shown. A. Chest CT scan shows diffusely scattered coarse calcifications and some internal fat density (arrow) in irradiated right breast. B. US image of right breast shows diffuse acoustic shadowing due to dense calcification with diffuse skin thickening, suggesting presence of radiation-induced changes.
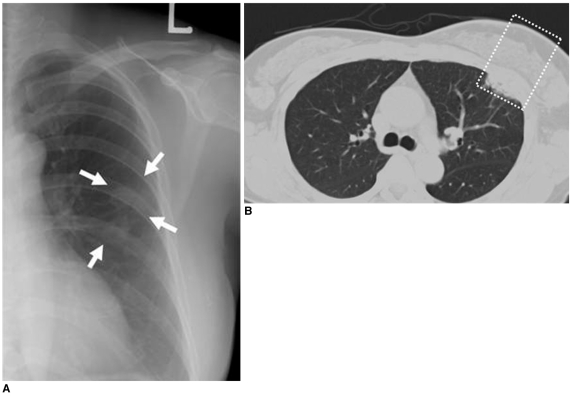
56-year-old female patient who had undergone radiation therapy in left breast eight months ago are shown. A. Chest radiograph shows circumscribed patchy consolidation (arrows) in left mid lung field. B. Chest CT scan demonstrates presence of sharply demarcated pneumonic consolidation in anterior aspect of left upper lobe along previous radiation field (box), suggesting presence of radiation-induced pneumonia.
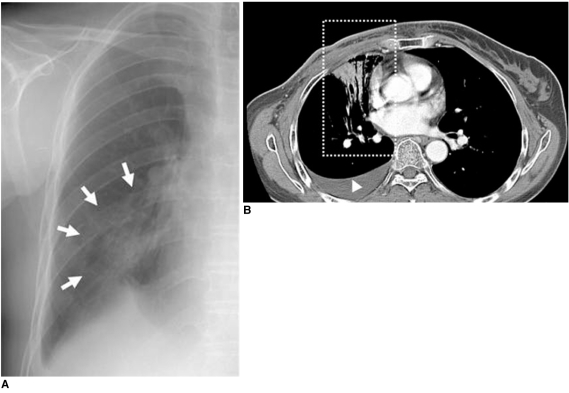
52-year-old female patient who had undergone radiation therapy in right breast two weeks ago are shown. A. Chest radiograph shows peribronchial consolidation in right mid lung field (arrows). B. Chest CT scan shows air-space consolidation with air-bronchogram localized in medial portion of right lung (box) that was related to previous radiation field for internal mammary lymph nodes, suggesting presence of radiation-induced pneumonia. Associated right pleural effusion is also noted (arrowhead).
36-year-old female patient who had undergone radiation therapy in right breast four years ago are shown. A. Initial postoperative mammogram obtained after six months shows diffuse skin and trabecular thickening, suggesting presence of radiation-induced breast edema. B, C. Annual follow-up mammograms show gradually decreased breast volume with diffusely increased glandular density due to progressive glandular atrophy with fibrosis.
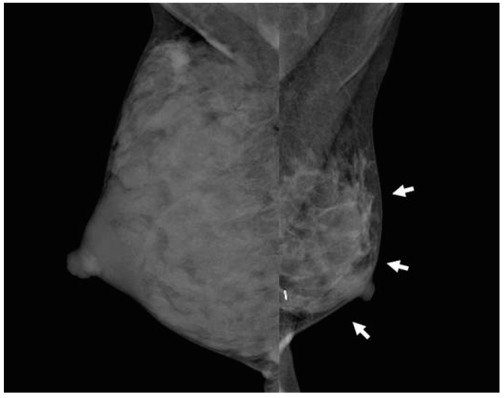
36-year-old female patient who had undergone radiation therapy in left breast three years ago are shown. Patient had breast-feeding difficulty in irradiated left breast. Mammography shows diffuse glandular atrophy (arrows) in irradiated left breast and compensatory glandular hypertrophy in right breast.
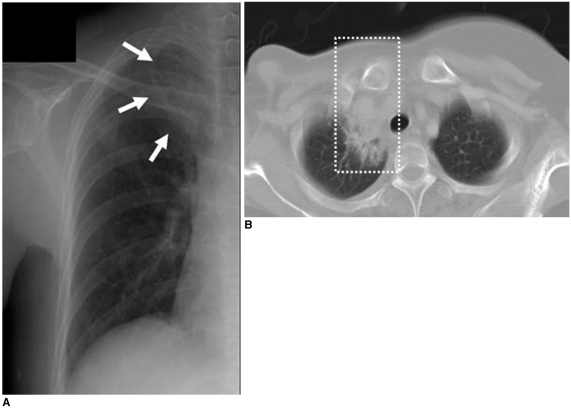
49-year-old female patient who had undergone radiation therapy in right breast three years ago are shown. A. Chest radiograph shows presence of localized fibrotic lesion in apical portion of right upper lobe (arrows). B. Chest CT scan shows fibrosis with bronchiectasis (box) localized in medial portion of right pulmonary apex that was associated with radiation therapy for right supraclavicular lymph nodes.
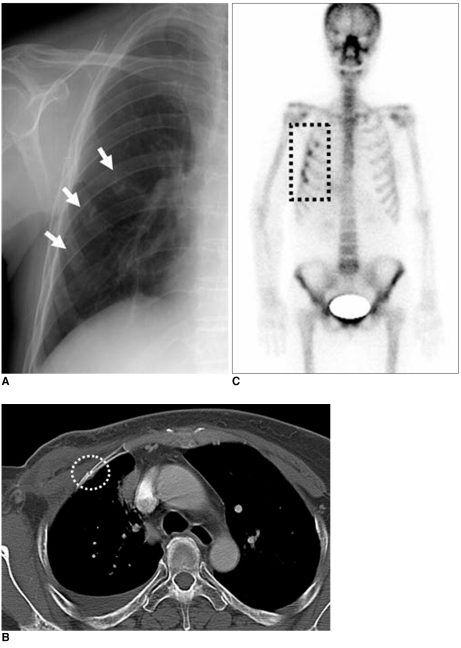
59-year-old female patient who had undergone radiation therapy in right breast six years ago are shown. A. Chest radiograph shows rib fractures involving right anterior chest wall (arrows). B. Chest CT scan shows relatively sharply defined fracture line without adjacent mass formation (circle). C. Bone scan shows multiple hot uptakes confined to anterior arcs of right ribs associated with radiation field (box).
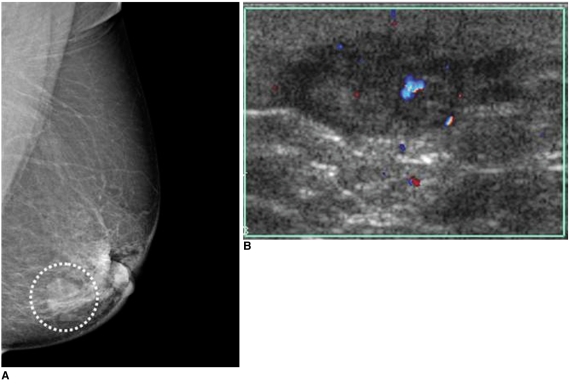
62-year-old female patient who had undergone left breast-conserving surgery that was followed by radiation therapy due to invasive ductal carcinoma six years ago are shown. A. Mammography of left breast shows mass with obscured margin, relatively round shape and isodensity in previous operation site (circle). B. Careful US study of left breast shows hypoechoic mass with microlobulated margin and irregular shape with increased vascularity, as seen on color Doppler US. Presence of radiation-induced angiosarcoma was confirmed after pathological examination. (Courtesy of Yeong-Mi Park, MD Inje University Pusan Paik Hospital and Ki-Seok Choo, MD, Pusan National University Hospital)
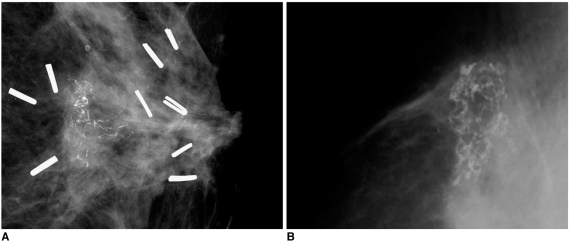
Examples of calcifications in previous operation bed are presented. A. 53-year-old female patient who had undergone left breast-conserving surgery that was followed by radiation therapy due to invasive ductal carcinoma eight months ago are shown. Mammography of left breast shows clustered microcalcifications with linear branching pattern and pleomorphism. Presence of recurrent ductal carcinoma in situ was confirmed after pathological examination. B. 68-year-old female patient who had undergone right breast-conserving surgery that was followed by radiation therapy due to invasive ductal carcinoma one year prior are shown. Mammography shows presence of lucent centered curvilinear calcifications without associated mass. Presence of fat necrosis was confirmed after pathological examination.
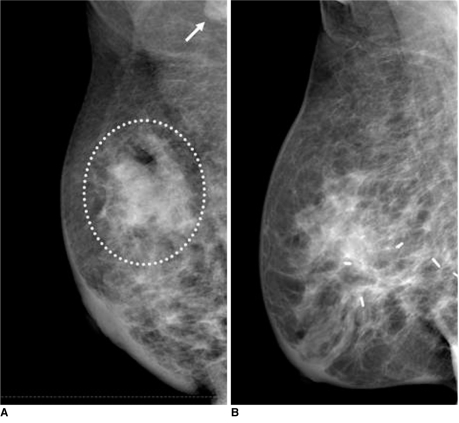
Examples of breast edema with skin thickening are presented. A. 45-year-old female patient who had diagnosed inflammatory breast cancer in right breast are shown. Mammography of right breast shows mass with indistinct margin, irregular shape and hyperdensity (circle). In addition, there is prominent metastatic lymph node located in right axilla (arrow). B. 49-year-old female patient who had radiation-induced breast edema associated with previous radiation therapy are shown. Mammography shows diffuse skin and trabecular thickening without definite mass lesion.
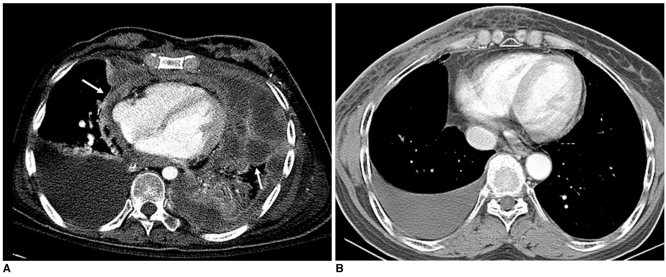
Examples of pleural effusion are presented. A. 53-year-old female patient who had undergone left conservation surgery due to invasive ductal carcinoma two years ago are shown. Chest CT scans show nodular seeding lesions along pleuropericardial surface (arrows) with malignant pleural effusion. B. Right pleural effusion without associated nodularity in 59-year-old female patient who was subjected to right breast irradiation two weeks prior is shown, suggesting presence of radiation-induced pleurisy.
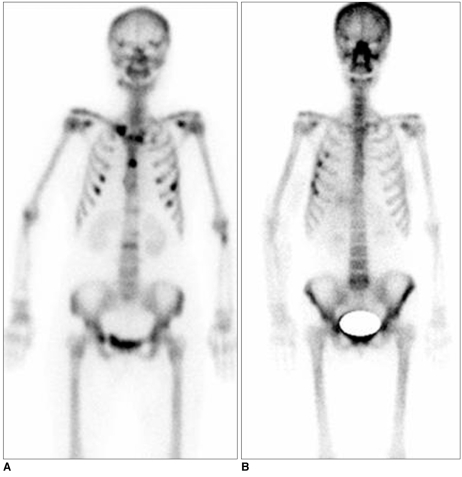
Examples of overlying bone lesions are presented. A. Multiple bone metastases are seen as multifocal hot uptake lesions without association of radiation field on bone scan. B. Radiation-induced bone fracture shows hot uptake lesions localized in overlying ribs associated with radiation field as depicted on bone scan.
References
-
- Sabin BM, Eric AS, Marsha DM, Thomas AB. Breast cancer. In: Levitt SH, Purdy JA, Perez CA, Vijayakumar S, editors. Technical basis of radiation therapy: practical clinical applications. 4th ed. Berlin: Baert AL; 2006. pp. 486–510.
-
- Coles CE, Moody AM, Wilson CB, Burnet NG. Reduction of radiotherapy-induced late complications in early breast cancer: the role of intensity-modulated radiation therapy and partial breast irradiation. Part I--normal tissue complications. Clin Oncol (R Coll Radiol) 2005;17:16–24. - PubMed
-
- Moore AH, Olschowka JA, Williams JP, Paige SL, O'Banion MK. Radiation-induced edema is dependent on cyclooxygenase 2 activity in mouse brain. Radiat Res. 2004;161:153–160. - PubMed
-
- Iwasaki H, Morimoto K, Koh M, Okamura T, Wakasa K, Wakasa T, et al. A case of fat necrosis after breast quadrantectomy in which preoperative diagnosis was enabled by MRI with fat suppression technique. Magn Reson Imaging. 2004;22:285–290. - PubMed
-
- Lind P. Clinical relevance of pulmonary toxicity in adjuvant breast cancer irradiation. Acta Oncol. 2006;54:13–15. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
