

Chlorhexidine, toothbrushing, and preventing ventilator-associated pneumonia in critically ill adults
- PMID: 19723863
- PMCID: PMC3722581
- DOI: 10.4037/ajcc2009792
Chlorhexidine, toothbrushing, and preventing ventilator-associated pneumonia in critically ill adults
Abstract
Background: Ventilator-associated pneumonia is associated with increased morbidity and mortality.
Objective: To examine the effects of mechanical (toothbrushing), pharmacological (topical oral chlorhexidine), and combination (toothbrushing plus chlorhexidine) oral care on the development of ventilator-associated pneumonia in critically ill patients receiving mechanical ventilation.
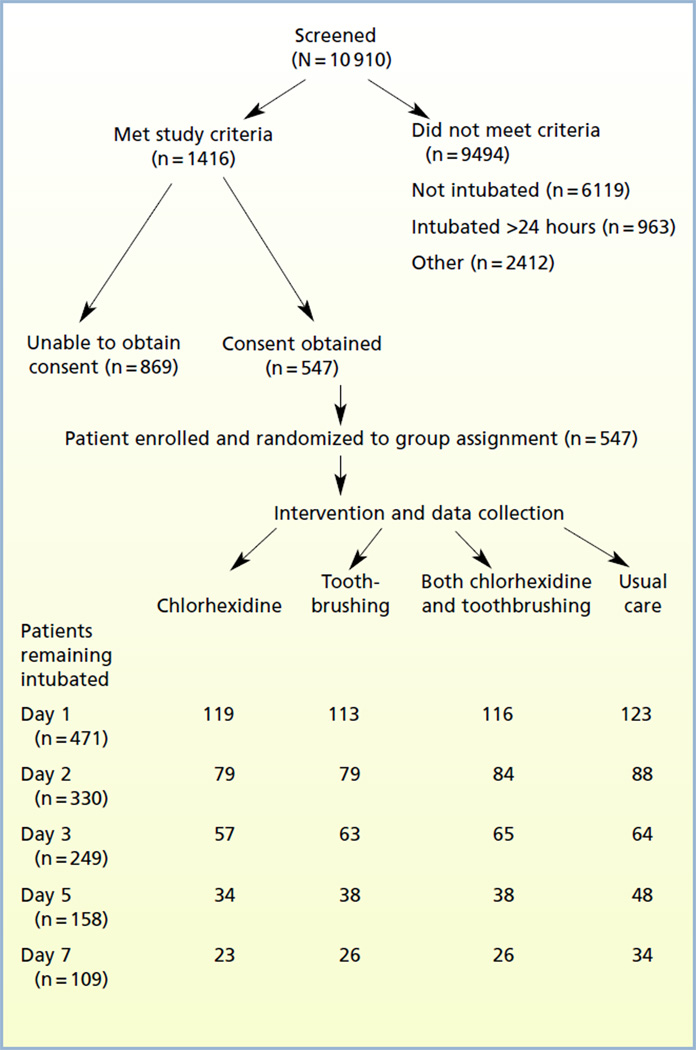
Methods: Critically ill adults in 3 intensive care units were enrolled within 24 hours of intubation in a randomized controlled clinical trial with a 2 x 2 factorial design. Patients with a clinical diagnosis of pneumonia at the time of intubation and edentulous patients were excluded. Patients (n = 547) were randomly assigned to 1 of 4 treatments: 0.12% solution chlorhexidine oral swab twice daily, toothbrushing thrice daily, both toothbrushing and chlorhexidine, or control (usual care). Ventilator-associated pneumonia was determined by using the Clinical Pulmonary Infection Score (CPIS).
Results: The 4 groups did not differ significantly in clinical characteristics. At day 3 analysis, 249 patients remained in the study. Among patients without pneumonia at baseline, pneumonia developed in 24% (CPIS >or=6) by day 3 in those treated with chlorhexidine. When data on all patients were analyzed together, mixed models analysis indicated no effect of either chlorhexidine (P = .29) or toothbrushing (P = .95). However, chlorhexidine significantly reduced the incidence of pneumonia on day 3 (CPIS >or=6) among patients who had CPIS <6 at baseline (P = .006). Toothbrushing had no effect on CPIS and did not enhance the effect of chlorhexidine.
Conclusions: Chlorhexidine, but not toothbrushing, reduced early ventilator-associated pneumonia in patients without pneumonia at baseline.
Comment in
-
Modest reduction in risk for ventilator-associated pneumonia in critically ill patients receiving mechanical ventilation following topical oral chlorhexidine.J Evid Based Dent Pract. 2012 Jun;12(2):103-6. doi: 10.1016/j.jebdp.2012.03.010. J Evid Based Dent Pract. 2012. PMID: 22726793 No abstract available.
-
Modest reduction in risk for ventilator-associated pneumonia in critically ill patients receiving mechanical ventilation following topical oral chlorhexidine.J Evid Based Dent Pract. 2012 Sep;12(3 Suppl):15-7. doi: 10.1016/S1532-3382(12)70004-0. J Evid Based Dent Pract. 2012. PMID: 23253825
References
-
- Cook D. Ventilator associated pneumonia: perspectives on the burden of illness. Intensive Care Med. 2000;26(suppl 1):S31–S37. - PubMed
-
- Byers JF, Sole ML. Analysis of factors related to the development of ventilator-associated pneumonia: use of existing databases. Am J Crit Care. 2000;9:344–349. - PubMed
-
- Rodriguez JL, Gibbons KJ, Bitzer LG, Dechert RE, Steinberg SM, Flint LM. Pneumonia: incidence, risk factors, and outcome in injured patients. J Trauma. 1991;31:907–912. - PubMed
-
- Leu HS, Kaiser DL, Mori M, Woolson RF, Wenzel RP. Hospital-acquired pneumonia: attributable mortality and morbidity. Am J Epidemiol. 1989;129:1258–1267. - PubMed
-
- Haley RW, Schaberg DR, Crossley K, Von Allmen SD, McGowan JE., Jr Extra charges and prolongation of stay attributable to nosocomial infections: a prospective inter-hospital comparison. Am J Med. 1981;70:51–58. - PubMed
