

Geographic mapping of meniscus and cartilage lesions associated with anterior cruciate ligament injuries
- PMID: 19723985
- PMCID: PMC7002077
- DOI: 10.2106/JBJS.H.00888
Geographic mapping of meniscus and cartilage lesions associated with anterior cruciate ligament injuries
Abstract
Background: Detailed descriptions of meniscus and articular cartilage lesions associated with anterior cruciate ligament injury have not been presented in the literature. Our goal was to determine the associations between patient sex, age, and surgical delay and the frequency and location of meniscus and articular cartilage lesions seen at the time of the anterior cruciate ligament reconstruction.
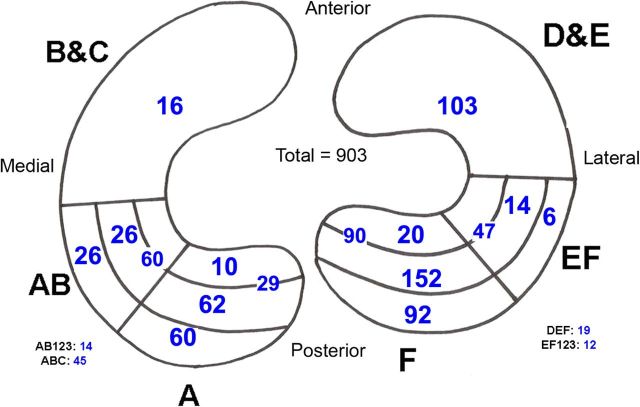
Methods: Data were obtained retrospectively from a database of 1209 consecutive patients undergoing anterior cruciate ligament reconstruction between 1988 and 2002. All knee cartilage, meniscus, and ligament injuries were documented on anatomic maps at the time of surgery, and the data were analyzed.
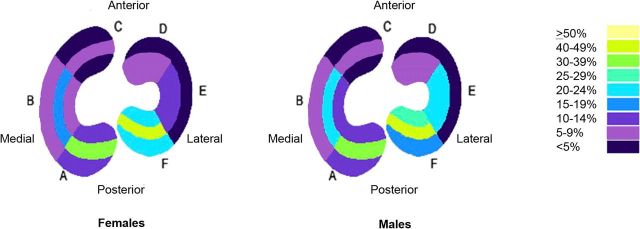
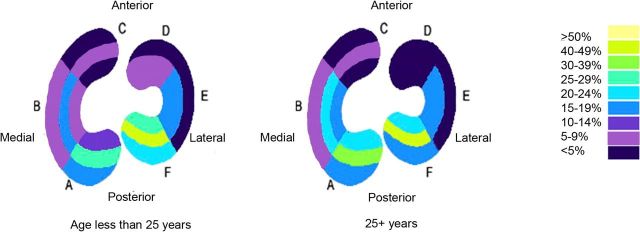
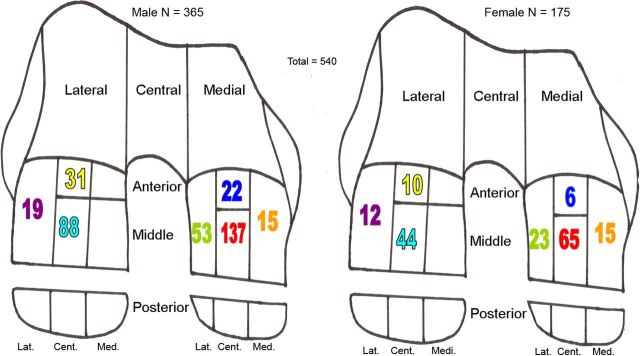
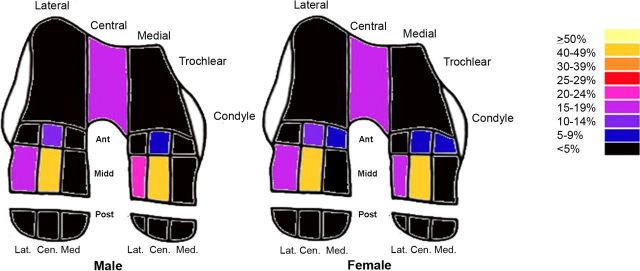
Results: Meniscus injuries were identified in 722 (65%) of the 1104 patients who met the criteria for inclusion in the study. Female patients were less likely to have a meniscus injury than male patients were (56% compared with 71%), and male patients were more likely to have combined medial and lateral meniscus injuries than female patients were (20% compared with 11%). Patients with a surgical delay of less than three months were less likely to have a medial meniscus injury (8% compared with 19%). Femoral articular cartilage injuries were identified in 472 patients (43%). Patients who were twenty-five years of age or older were more likely to have multiple cartilage lesions throughout the knee (7.7% compared with 1.3%) and to have more isolated medial femoral condyle lesions (24.2% compared with 13.3%). Patients with a surgical delay of more than one year were more likely to have a lesion (60% compared with 47% for all others), and a surgical delay of more than one year resulted in a greater proportion of large and grade-3 lesions of the lateral femoral condyle. Female patients had a greater proportion of grade-1 lesions of the medial femoral condyle (29% compared with 16%), whereas male patients had a greater proportion of grade-3 and 4 lesions of the medial femoral condyle (49% compared with 35%). In patients who were thirty-five years of age or older, meniscus injuries were more frequent and were located more frequently on the medial side; femoral articular cartilage lesions were also located more frequently on the medial side.
Conclusions: Increased age, male sex, and increased surgical delay all increase the frequency and severity of injuries of the meniscus and/or articular cartilage after an anterior cruciate ligament tear.
Figures



References
-
- Kaeding CC, Pedroza AD, Parker RD, Spindler KP, McCarthy EC, Andrish JT. Intra-articular findings in the reconstructed multiligament-injured knee. Arthroscopy. 2005;21:424-30. - PubMed
-
- Maffulli N, Binfield PM, King JB. Articular cartilage lesions in the symptomatic anterior cruciate ligament-deficient knee. Arthroscopy. 2003;19:685-90. - PubMed
-
- Murrell GA, Maddali S, Horovitz L, Oakley SP, Warren RF. The effects of time course after anterior cruciate ligament injury in correlation with meniscal and cartilage loss. Am J Sports Med. 2001;29:9-14. - PubMed
-
- O'Connor DP, Laughlin MS, Woods GW. Factors related to additional knee injures after anterior cruciate ligament injury. Arthroscopy. 2005;21:431-8. - PubMed
-
- Piasecki DP, Spindler KP, Warren TA, Andrish JT, Parker RD. Intraarticular injuries associated with anterior cruciate ligament tear: findings at ligament reconstruction in high school and recreational athletes. An analysis of sex-based differences. Am J Sports Med. 2003;31:601-5. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
