

Iatrogenic bile duct injuries: etiology, diagnosis and management
- PMID: 19725140
- PMCID: PMC2738802
- DOI: 10.3748/wjg.15.4097
Iatrogenic bile duct injuries: etiology, diagnosis and management
Abstract
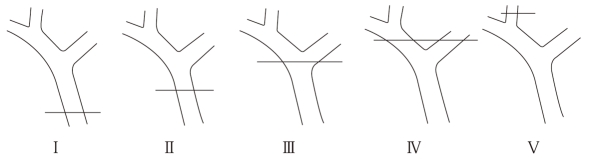
Iatrogenic bile duct injuries (IBDI) remain an important problem in gastrointestinal surgery. They are most frequently caused by laparoscopic cholecystectomy which is one of the commonest surgical procedures in the world. The early and proper diagnosis of IBDI is very important for surgeons and gastroenterologists, because unrecognized IBDI lead to serious complications such as biliary cirrhosis, hepatic failure and death. Laboratory and radiological investigations play an important role in the diagnosis of biliary injuries. There are many classifications of IBDI. The most popular and simple classification of IBDI is the Bismuth scale. Endoscopic techniques are recommended for initial treatment of IBDI. When endoscopic treatment is not effective, surgical management is considered. Different surgical reconstructions are performed in patients with IBDI. According to the literature, Roux-en-Y hepaticojejunostomy is the most frequent surgical reconstruction and recommended by most authors. In the opinion of some authors, a more physiological and equally effective type of reconstruction is end-to-end ductal anastomosis. Long term results are the most important in the assessment of the effectiveness of IBDI treatment. There are a few classifications for the long term results in patients treated for IBDI; the Terblanche scale, based on clinical biliary symptoms, is regarded as the most useful classification. Proper diagnosis and treatment of IBDI may avoid many serious complications and improve quality of life.
Figures
References
-
- Negi SS, Sakhuja P, Malhotra V, Chaudhary A. Factors predicting advanced hepatic fibrosis in patients with postcholecystectomy bile duct strictures. Arch Surg. 2004;139:299–303. - PubMed
-
- Pellegrini CA, Thomas MJ, Way LW. Recurrent biliary stricture. Patterns of recurrence and outcome of surgical therapy. Am J Surg. 1984;147:175–180. - PubMed
-
- Tocchi A, Mazzoni G, Liotta G, Costa G, Lepre L, Miccini M, De Masi E, Lamazza MA, Fiori E. Management of benign biliary strictures: biliary enteric anastomosis vs endoscopic stenting. Arch Surg. 2000;135:153–157. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
