

Prospective validation of the ICH Score for 12-month functional outcome
- PMID: 19726752
- PMCID: PMC2764394
- DOI: 10.1212/WNL.0b013e3181b8b332
Prospective validation of the ICH Score for 12-month functional outcome
Abstract
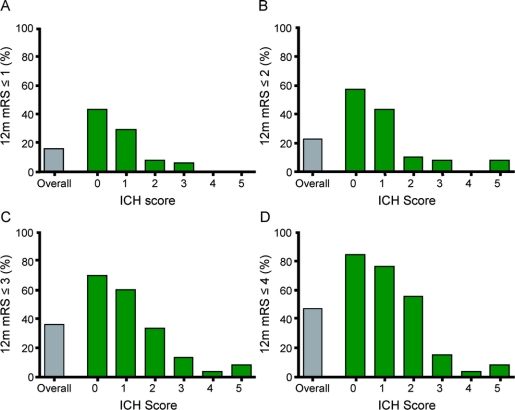
Background: The ICH Score is a commonly used clinical grading scale for outcome after acute intracerebral hemorrhage (ICH) and has been validated for 30-day mortality, but not long-term functional outcome. The goals of this study were to assess whether the ICH Score accurately stratifies patients with regard to 12-month functional outcome and to further delineate the pace of recovery of patients during the first year post-ICH.
Methods: We performed a prospective observational cohort study of all patients with acute ICH admitted to the emergency departments of San Francisco General Hospital and UCSF Medical Center from June 1, 2001, through May 31, 2004. Components of the ICH Score (admission Glasgow Coma Scale score, initial hematoma volume, presence of intraventricular hemorrhage, infratentorial ICH origin, and age) were recorded along with other clinical characteristics. Patients were then assessed with the modified Rankin Scale (mRS) at hospital discharge, 30 days, and 3, 6, and 12 months post-ICH.
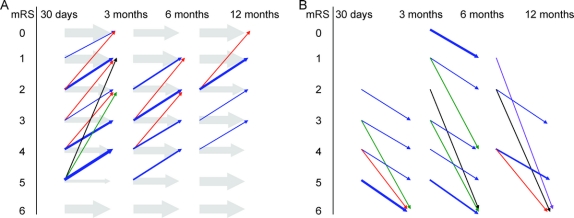
Results: Of 243 patients, 95 (39%) died during initial acute hospitalization. The ICH Score accurately stratified patients with regard to 12-month functional outcome for various dichotomous cutpoints along the mRS (p < 0.05). Many patients continued to improve across the first year, with a small number of patients becoming disabled or dying due to late events unrelated to the initial ICH.
Conclusions: The ICH Score is a valid clinical grading scale for long-term functional outcome after acute intracerebral hemorrhage (ICH). Many ICH patients improve after hospital discharge and this improvement may continue even after 6 months post-ICH.
Figures
Comment in
-
Improving stroke prognosis.Neurology. 2009 Oct 6;73(14):1084-5. doi: 10.1212/WNL.0b013e3181bc6747. Epub 2009 Sep 2. Neurology. 2009. PMID: 19726749 No abstract available.
References
-
- Hemphill JC 3rd, Bonovich DC, Besmertis L, Manley GT, Johnston SC. The ICH score: a simple, reliable grading scale for intracerebral hemorrhage. Stroke 2001;32:891–897. - PubMed
-
- Cheung RT, Zou LY. Use of the original, modified, or new intracerebral hemorrhage score to predict mortality and morbidity after intracerebral hemorrhage. Stroke 2003;34:1717–1722. - PubMed
-
- Clarke JL, Johnston SC, Farrant M, Bernstein R, Tong D, Hemphill JC 3rd. External validation of the ICH score. Neurocrit Care 2004;1:53–60. - PubMed
-
- Fernandes H, Gregson BA, Siddique MS, Mendelow AD. Testing the ICH score. Stroke 2002;33:1455–1456. - PubMed
-
- Jamora RD, Kishi-Generao EM, Jr., Bitanga ES, Gan RN, Apaga NE, San Jose MC. The ICH score: predicting mortality and functional outcome in an Asian population. Stroke 2003;34:6–7. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical