

Ubiquitin C-terminal hydrolase is a novel biomarker in humans for severe traumatic brain injury
- PMID: 19726976
- PMCID: PMC3445330
- DOI: 10.1097/CCM.0b013e3181b788ab
Ubiquitin C-terminal hydrolase is a novel biomarker in humans for severe traumatic brain injury
Abstract
Objective: Ubiquitin C-terminal hydrolase (UCH-L1), also called neuronal-specific protein gene product (PGP 9.3), is highly abundant in neurons. To assess the reliability of UCH-L1 as a potential biomarker for traumatic brain injury (TBI) this study compared cerebrospinal fluid (CSF) levels of UCH-L1 from adult patients with severe TBI to uninjured controls; and examined the relationship between levels with severity of injury, complications and functional outcome.
Design: This study was designed as prospective case control study.
Patients: This study enrolled 66 patients, 41 with severe TBI, defined by a Glasgow coma scale (GCS) score of < or =8, who underwent intraventricular intracranial pressure monitoring and 25 controls without TBI requiring CSF drainage for other medical reasons.
Setting: : Two hospital system level I trauma centers.
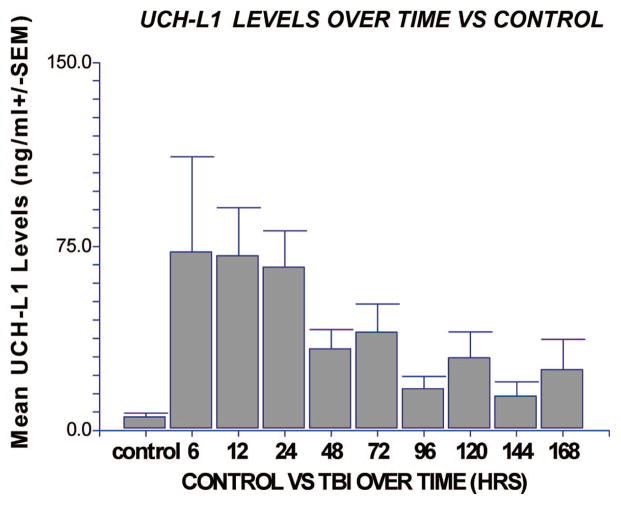
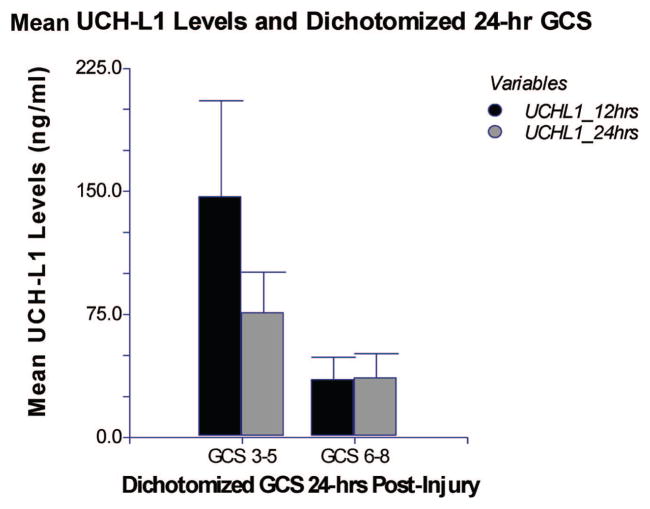
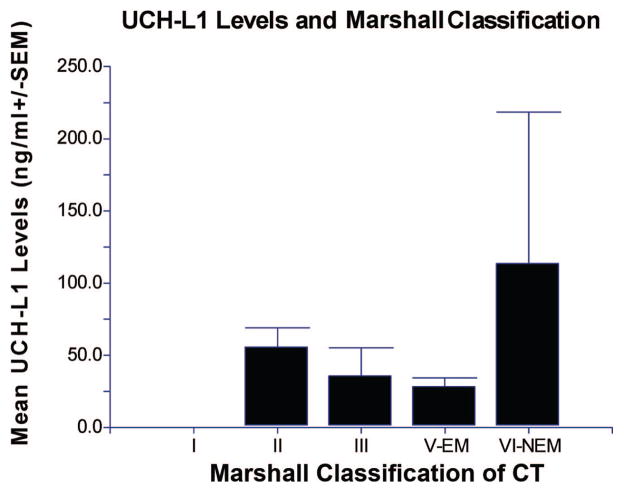
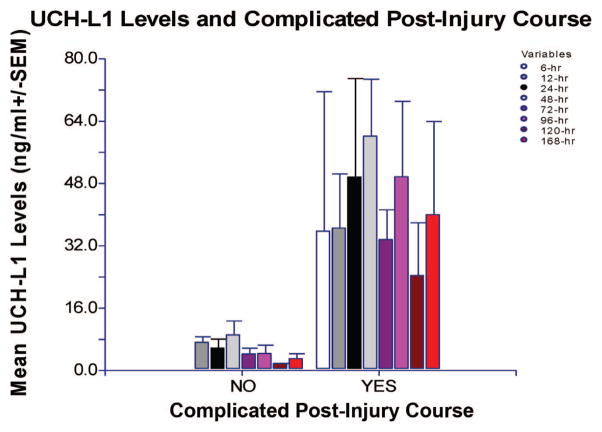
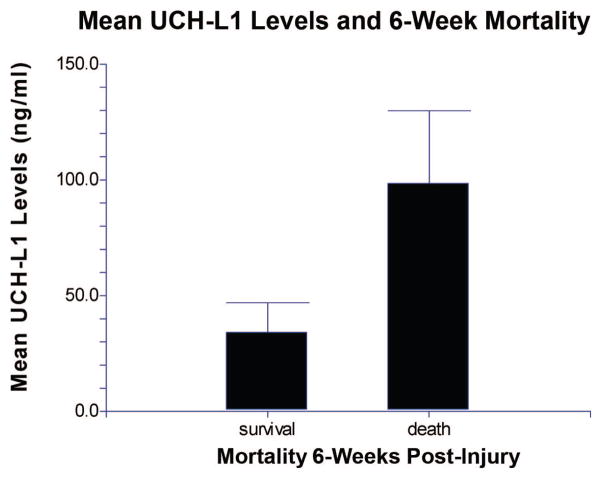
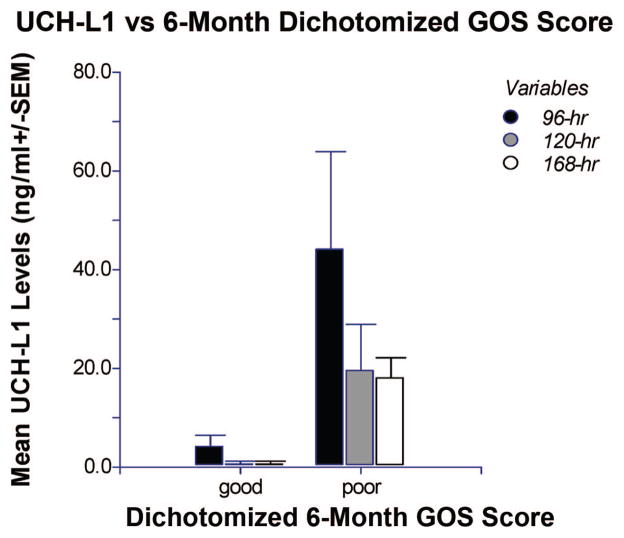
Measurements and main results: Ventricular CSF was sampled from each patient at 6, 12, 24, 48, 72, 96, 120, 144, and 168 hrs following TBI and analyzed for UCH-L1. Injury severity was assessed by the GCS score, Marshall Classification on computed tomography and a complicated postinjury course. Mortality was assessed at 6 wks and long-term outcome was assessed using the Glasgow outcome score 6 months after injury. TBI patients had significantly elevated CSF levels of UCH-L1 at each time point after injury compared to uninjured controls. Overall mean levels of UCH-L1 in TBI patients was 44.2 ng/mL (+/-7.9) compared with 2.7 ng/mL (+/-0.7) in controls (p <.001). There were significantly higher levels of UCH-L1 in patients with a lower GCS score at 24 hrs, in those with postinjury complications, in those with 6-wk mortality, and in those with a poor 6-month dichotomized Glasgow outcome score.
Conclusions: These data suggest that this novel biomarker has the potential to determine injury severity in TBI patients. Further studies are needed to validate these findings in a larger sample.
Conflict of interest statement
Drs. Papa, Hayes, and Wang are consultants for Banyan Biomarkers. The remaining authors have not disclosed any potential conflicts of interest.
Figures
Comment in
-
The race for biomarkers in traumatic brain injury: what science promises and the clinicians still expect.Crit Care Med. 2010 Jan;38(1):318-9. doi: 10.1097/CCM.0b013e3181b9d5ac. Crit Care Med. 2010. PMID: 20023481 No abstract available.
References
-
- Consensus conference. Rehabilitation of persons with traumatic brain injury. NIH Consensus Development Panel on Rehabilitation of Persons With Traumatic Brain Injury. JAMA. 1999;282:974–983. - PubMed
-
- Doppenberg EM, Choi SC, Bullock R. Clinical trials in traumatic brain injury: Lessons for the future. J Neurosurg Anesthesiol. 2004;16:87–94. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
