

Microvasculitis in diabetic lumbosacral radiculoplexus neuropathy
- PMID: 19730021
- PMCID: PMC2786308
- DOI: 10.1097/CND.0b013e3181b1eb6d
Microvasculitis in diabetic lumbosacral radiculoplexus neuropathy
Abstract
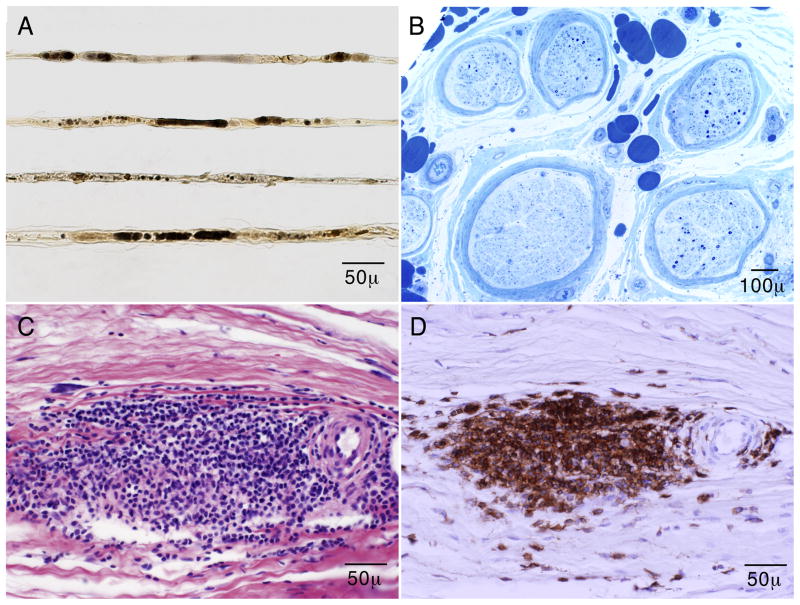
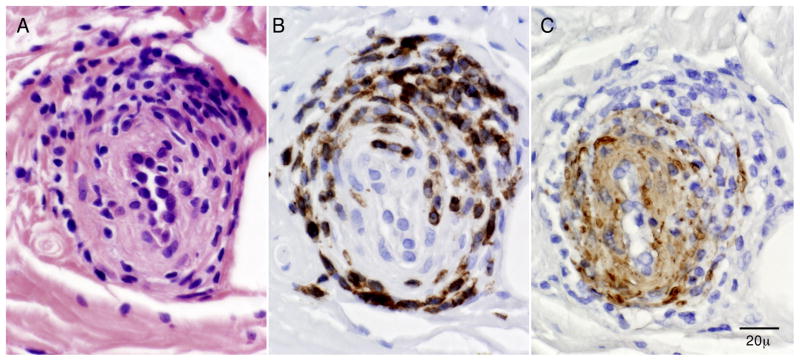
We present a case of a 60-year-old man with mild type 2 diabetes mellitus and step-wise progression of bilateral lower limb weakness, numbness, and pain over a 1-year period. At the time of evaluation, he used a walker. He had elevated cerebrospinal fluid protein, abnormal cooling and heat-pain thresholds on quantitative sensory testing, and nerve conduction studies/electromyography consistent with bilateral lumbosacral radiculoplexus neuropathies. Because it was not clear whether the disease was still active, a right superficial peroneal nerve biopsy was performed and showed evidence of active axonal degeneration, ischemic injury, and microvasculitis. On the basis of these results, the patient was diagnosed with diabetic lumbosacral radiculoplexus neuropathy and was treated with weekly intravenous methylprednisolone with marked improvement of neurologic symptoms and signs. This case illustrates the typical clinical, electrophysiologic, and pathologic features of diabetic lumbosacral radiculoplexus neuropathy and the utility of nerve biopsy to judge ongoing disease activity.
Figures
References
-
- Dyck PJ, Zimmerman IR, O’Brien PC, et al. Introduction of automated systems to evaluate touch-pressure, vibration, and thermal cutaneous sensation in man. Ann Neurol. 1978;4:502–510. - PubMed
-
- Dyck PJ, Zimmerman I, Gillen DA, Johnson D, Karnes JL, O’Brien PC. Cool, warm, and heat-pain detection of receptors: testing methods and inferences about anatomic distribution of receptors. Neurology. 1993;43:1500–1508. - PubMed
-
- Bastron JA, Thomas JE. Diabetic polyradiculopathy: clinical and electromyographic findings in 105 patients. Mayo ClinProc. 1981;56:725–732. - PubMed
-
- Williams IR, Mayer RF. Subacute proximal diabetic neuropathy. Neurology. 1976;26:108–116. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
