

Effect of epsilon aminocaproic acid on red-cell transfusion requirements in major spinal surgery
- PMID: 19730217
- PMCID: PMC2772136
- DOI: 10.1097/BRS.0b013e3181b1fab2
Effect of epsilon aminocaproic acid on red-cell transfusion requirements in major spinal surgery
Abstract
Study design: : Randomized, placebo-controlled trial.
Objective: : To evaluate the efficacy of epsilon aminocaproic acid (EACA) to reduce the number of red-cell (RBC) transfusions in adult patients undergoing major spinal surgery.
Summary of background data: : Reconstructive spinal surgery is associated with significant blood loss. The number of studies evaluating the efficacy of EACA in adult patients undergoing spinal surgery remains scarce and limited.
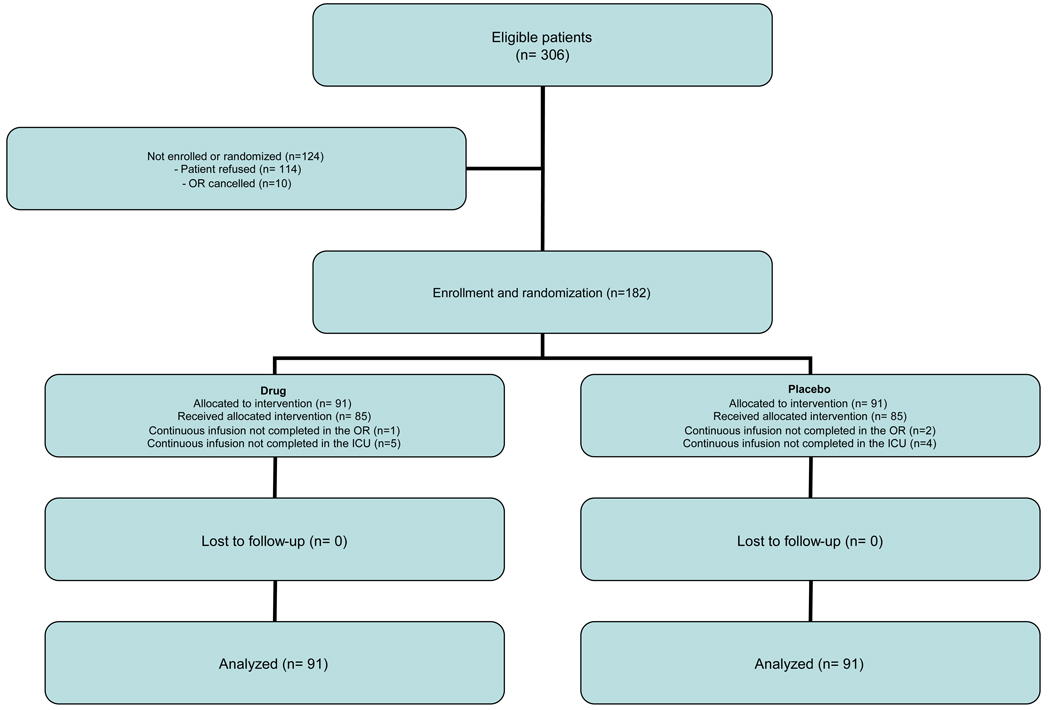
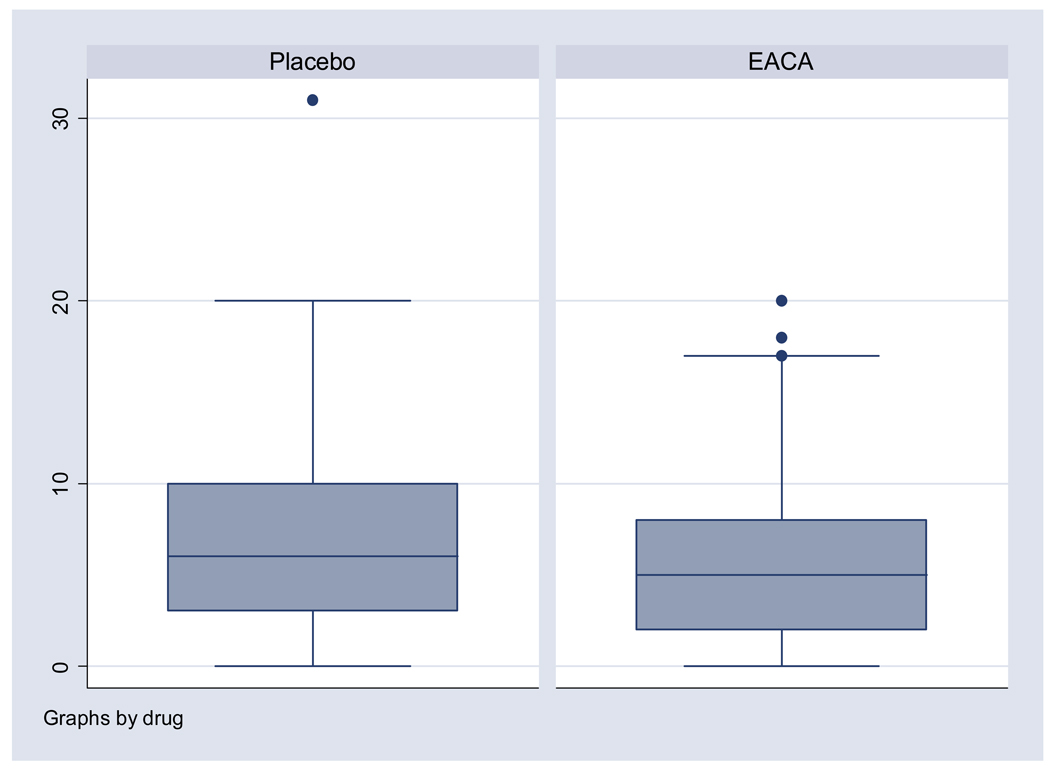
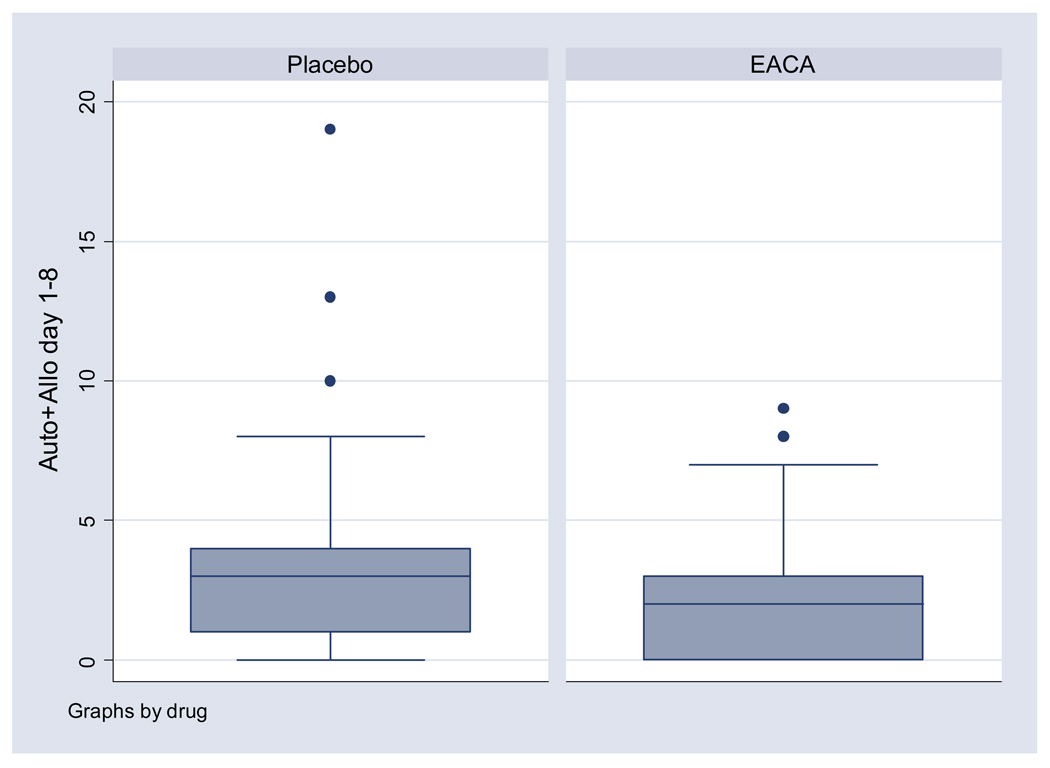
Methods: : EACA (100 mg/kg) or placebo was administered to 182 adult patients after the induction of anesthesia followed by an infusion that was continued for 8 hours after surgery. Primary end points included total allogeneic RBC transfusions through postoperative day 8 and postoperative allogeneic plus autologus RBC transfusions through postoperative day 8.
Results: : Mean total allogeneic RBC transfusions were not statistically different between the groups (5.9 units EACA vs. 6.9 units placebo; P = 0.17). Mean postoperative RBC transfusions in the EACA group was less (2.0 units vs. 2.8 units placebo; P = 0.03). There was no significantdifference in mean estimated intraoperative estimated-blood loss (2938 cc EACA vs. 3273 cc placebo; P = 0.32). Mean intensive care unit length of stay was decreased (EACA: 1.8 days vs. 2.8 days placebo; P = 0.04). The incidence of thromboembolic complications was similar (2.2% EACA vs. 6.6% placebo; P = 0.15).
Conclusion: : The difference in total allogeneic RBC transfusions between the groups was not statistically significant. EACA was associated with a 30% (0.8 units) reduction in postoperative RBC transfusions and a 1-day reduction in ICU LOS, without an increased incidence of thromboembolic events. EACA may be considered for patients undergoing major spinal surgery. Larger studies are needed to evaluate the relationship between EACA and total RBC requirements.
Trial registration: ClinicalTrials.gov NCT00320619.
Figures
References
-
- Goodnough LT, Brecher ME, Kanter MH, AuBuchon JP. Transfusion Medicine. First of two parts: Blood transfusion. NEJM. 1999;340(6):438–447. - PubMed
-
- Blajchman MA, Vamvakas EC. The continuing risk of transfusion-transmitted infections. N Engl J Med. 2006;355:1303–1305. - PubMed
-
- Spahn DR, Casutt M. Eliminating blood transfusions: New aspects and perspectives. Anesthesiology. 2000;93(1):242–255. - PubMed
-
- Mannucci PM, Levi M. Prevention and Treatment of Major Blood Loss. N Engl J Med. 2007;356:2301–2311. - PubMed
-
- Henry DA, Carless PA, Moxey AJ, O’Connell D, Stokes BJ, McClelland B, Laupacis A, Fergusson D. Anti-fibrinolytic use for minimising perioperative allogeneic blood transfusion. Cochrane Database Syst Rev. 2007;17(4) CD001886. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
