

Perthes disease: current principles of diagnosis and treatment
- PMID: 19730720
- PMCID: PMC2735835
- DOI: 10.3238/arztebl.2009.0517
Perthes disease: current principles of diagnosis and treatment
Abstract
Background: Because the course of Legg-Calvé-Perthes disease (LCPD) is highly variable, its appropriate diagnostic evaluation and treatment are still debated.
Methods: The authors selectively review the literature, present their own study findings, and discuss the guidelines of the German Society for Orthopedics and Orthopedic Surgery.
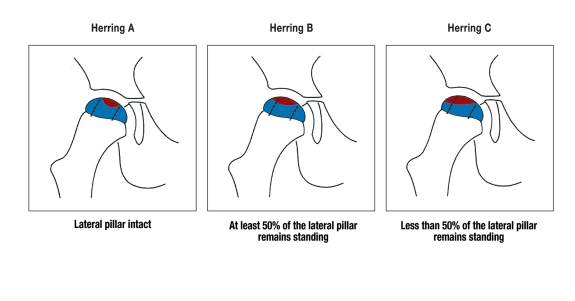
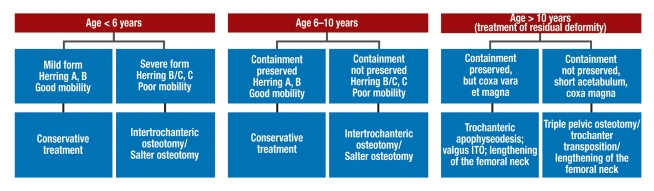
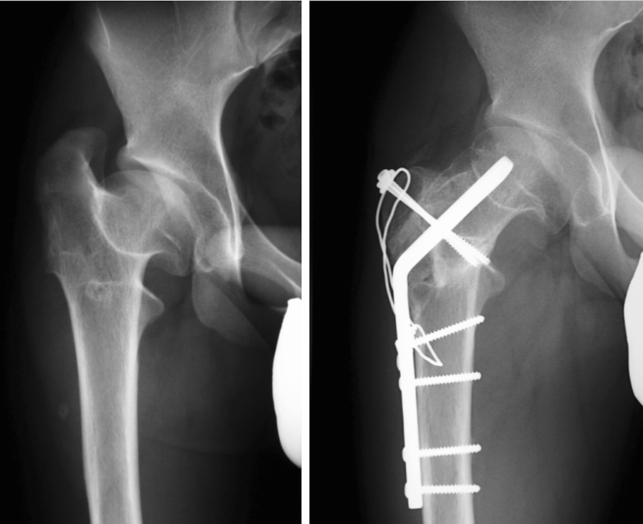
Results: The main prognostic factors are the patient's age at the onset of the disease, the degree of limitation of range of motion, the extent of involvement of the femoral epiphysis, and any additional radiographic "head-at-risk" signs. Depending on the severity of the disease, the treatment options range from observation and frequent follow-up to reconstructive hip surgery. The goal of all treatments is to prevent a prearthrotic deformity and the ensuing premature coxarthrosis. This goal is best met by adherence to the principle of containment, i.e., the maintenance or restoration of joint congruence while biological plasticity is still present.
Conclusions: In view of the variable course of LCPD, the proper course of treatment must be determined individually in each case. Every child with LCPD must receive individually adapted treatment and continued follow-up into adulthood.
Keywords: Legg-Calvé-Perthes disease; joint diagnosis; osteochondrosis; pediatric disease; prognosis.
Figures


Comment in
-
Alternative to crutches?Dtsch Arztebl Int. 2010 Jan;107(4):62; author reply 62. doi: 10.3238/arztebl.2010.0062a. Epub 2010 Jan 29. Dtsch Arztebl Int. 2010. PMID: 20165709 Free PMC article. No abstract available.
References
-
- Loder RT, Schwartz EM, Hensinger RN. Behavioral characteristics of children with Legg-Calvé-Perthes disease. J Pediatr Orthop. 1993;13:598–601. - PubMed
-
- Krauspe R, Raab P. Morbus Perthes. Orthopäde. 1997;26:289–302. - PubMed
-
- Eggl H, Drekonja T, Kaiser B, Dorn U. Ultrasonography in the diagnosis of transient synovitis of the hip and Legg-Calvé-Perthes disease. J Pediatr Orthop B. 1999;8(3):177–180. - PubMed
-
- Hefti F. Kinderorthopädie in der Praxis. 2. Aufl. Berlin, Heidelberg, New York: Springer; 2006.
-
- Thompson GH, Price CT, Roy D, Meehan PL, Richards BS. Legg-Calvé-Perthes disease AAOS. In: Birch JG, editor. Instructional Course Lectures. Rosemont: American Academy of Orthopedic Surgeons; 2006. pp. 27–44.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous