

Learning by doing, scale effects, or neither? Cardiac surgeons after residency
- PMID: 19732169
- PMCID: PMC2796309
- DOI: 10.1111/j.1475-6773.2009.01018.x
Learning by doing, scale effects, or neither? Cardiac surgeons after residency
Abstract
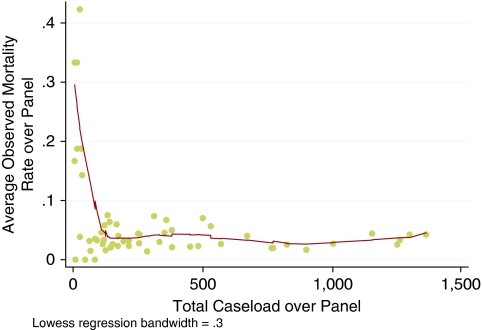
Objective: To examine impacts of operating surgeon scale and cumulative experience on postoperative outcomes for patients treated with coronary artery bypass grafts (CABG) by "new" surgeons. Pooled linear, fixed effects panel, and instrumented regressions were estimated.
Data sources: The administrative data included comorbidities, procedures, and outcomes for 19,978 adult CABG patients in Florida in 1998-2006, and public data on 57 cardiac surgeons who completed residencies after 1997.
Study design: Analysis was at the patient level. Controls for risk, hospital scale and scope, and operating surgeon characteristics were made. Patient choice model instruments were constructed. Experience was estimated allowing for "forgetting" effects.
Principal findings: Panel regressions with surgeon fixed effects showed neither surgeon scale nor cumulative volumes significantly impacted mortality nor consistently impacted morbidity. Estimation of "forgetting" suggests that almost all prior experience is depreciated from one quarter to the next. Instruments were strong, but exogeneity of volume was not rejected.
Conclusions: In postresidency surgeons, no persuasive evidence is found for learning by doing, scale, or selection effects. More research is needed to support the cautious view that, for these "new" cardiac surgeons, patient volume could be redistributed based on realized outcomes without disruption.
Figures
Similar articles
-
Outcomes of concomitant aortic valve replacement and coronary artery bypass grafting at teaching hospitals versus nonteaching hospitals.J Thorac Cardiovasc Surg. 2012 Mar;143(3):648-55. doi: 10.1016/j.jtcvs.2011.04.041. Epub 2011 Jun 30. J Thorac Cardiovasc Surg. 2012. PMID: 21719032
-
Cumulative team experience matters more than individual surgeon experience in cardiac surgery.J Thorac Cardiovasc Surg. 2013 Feb;145(2):328-33. doi: 10.1016/j.jtcvs.2012.09.022. Epub 2012 Oct 18. J Thorac Cardiovasc Surg. 2013. PMID: 23083794
-
The implication of seniority of supervising attending surgeon on the reexploration rate following elective coronary artery bypass grafting.J Formos Med Assoc. 2019 Jan;118(1 Pt 2):354-361. doi: 10.1016/j.jfma.2018.06.007. Epub 2018 Jun 20. J Formos Med Assoc. 2019. PMID: 29936106
-
The impact of short breaks from cardiac surgery on mortality and stay length in California.J Healthc Qual. 2014 Sep-Oct;36(5):42-9. doi: 10.1111/jhq.12018. Epub 2013 Jun 17. J Healthc Qual. 2014. PMID: 23773602
-
Characterizing the Operative Experience of Cardiac Surgical Trainees: What Are Residents Really Doing in the Operating Room?Ann Thorac Surg. 2016 Jun;101(6):2341-9. doi: 10.1016/j.athoracsur.2015.12.069. Epub 2016 Mar 26. Ann Thorac Surg. 2016. PMID: 27021035
Cited by
-
Renal transplantation: relationship between hospital/surgeon volume and postoperative severe sepsis/graft-failure. a nationwide population-based study.Int J Med Sci. 2014 Jun 24;11(9):918-24. doi: 10.7150/ijms.8850. eCollection 2014. Int J Med Sci. 2014. PMID: 25013372 Free PMC article.
-
Measuring the Volume-Outcome Relation for Complex Hospital Surgery.Appl Health Econ Health Policy. 2016 Aug;14(4):453-464. doi: 10.1007/s40258-016-0241-6. Appl Health Econ Health Policy. 2016. PMID: 27083171 Free PMC article.
-
Association of Surgeon Age and Experience With Congenital Heart Surgery Outcomes.Circ Cardiovasc Qual Outcomes. 2017 Jul;10(7):e003533. doi: 10.1161/CIRCOUTCOMES.117.003533. Circ Cardiovasc Qual Outcomes. 2017. PMID: 28710297 Free PMC article.
-
Association between physicians' experience after training and maternal obstetrical outcomes: cohort study.BMJ. 2013 Mar 28;346:f1596. doi: 10.1136/bmj.f1596. BMJ. 2013. PMID: 23538919 Free PMC article.
-
Practice variation, bias, and experiential learning in cesarean delivery: a data-based system dynamics approach.Health Serv Res. 2013 Apr;48(2 Pt 2):713-34. doi: 10.1111/1475-6773.12040. Epub 2013 Feb 10. Health Serv Res. 2013. PMID: 23398502 Free PMC article.
References
-
- Birkmeyer JD, Stukel TA, Siewers AE, Goodney PP, Wennberg DE, Lucas FL. Surgeon Volume and Operative Mortality in the United States. New England Journal of Medicine. 2003;349:2117–2. - PubMed
-
- Bonchek LI. Off-Pump Coronary Bypass: Is It for Everyone? Journal of Thoracic and Cardiovascular Surgery. 2002;124:431–4. - PubMed
-
- Bridgewater B, Grayson AD, Au J, Hassan R, Dihmis WC, Munsch C, Waterworth P. Improving Mortality of Coronary Surgery over First Four Years of Independent Practice: Retrospective Examination of Prospectively Collected Data from 15 Surgeons. British Medical Journal. 2004;329(7463):421. - PMC - PubMed
-
- California Office of Statewide Health Planning and Development. “The California Report on Coronary Artery Bypass Graft Surgery 2003–2004 Hospital and Surgeon Data” [accessed on March 3, 2008]. Available at http://www.oshpd.ca.gov/HID/Products/PatDischargeData/CABG/03-04fullrepo....
-
- Chernew ME, Gowrisankaran G, Fendrick AM. Payer Type and the Returns to Bypass Surgery: Evidence from Hospital Entry Behavior. Journal of Health Economics. 2002;21(3):451–74. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
