

Randomized controlled trial to determine the efficacy of long-term growth hormone treatment in severely burned children
- PMID: 19734776
- PMCID: PMC3970433
- DOI: 10.1097/SLA.0b013e3181b8f9ca
Randomized controlled trial to determine the efficacy of long-term growth hormone treatment in severely burned children
Abstract
Background: Recovery from a massive burn is characterized by catabolic and hypermetabolic responses that persist up to 2 years and impair rehabilitation and reintegration. The objective of this study was to determine the effects of long-term treatment with recombinant human growth hormone (rhGH) on growth, hypermetabolism, body composition, bone metabolism, cardiac work, and scarring in a large prospective randomized single-center controlled clinical trial in pediatric patients with massive burns.
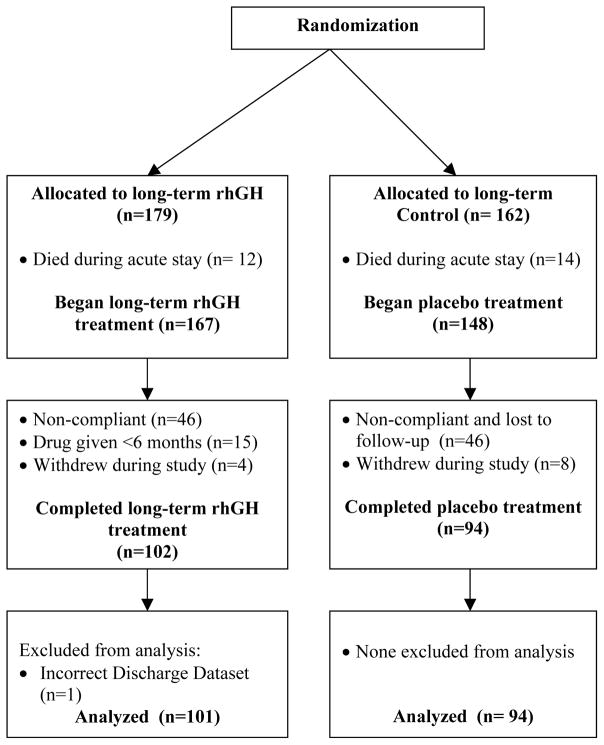
Patients and methods: A total of 205 pediatric patients with massive burns over 40% total body surface area were prospectively enrolled between 1998 and 2007 (clinicaltrials.gov ID NCT00675714). Patients were randomized to receive either placebo (n = 94) or long-term rhGH at 0.05, 0.1, or 0.2 mg/kg/d (n = 101). Changes in weight, body composition, bone metabolism, cardiac output, resting energy expenditure, hormones, and scar development were measured at patient discharge and at 6, 9, 12, 18, and 24 months postburn. Statistical analysis used Tukey t test or ANOVA followed by Bonferroni correction. Significance was accepted at P < 0.05.
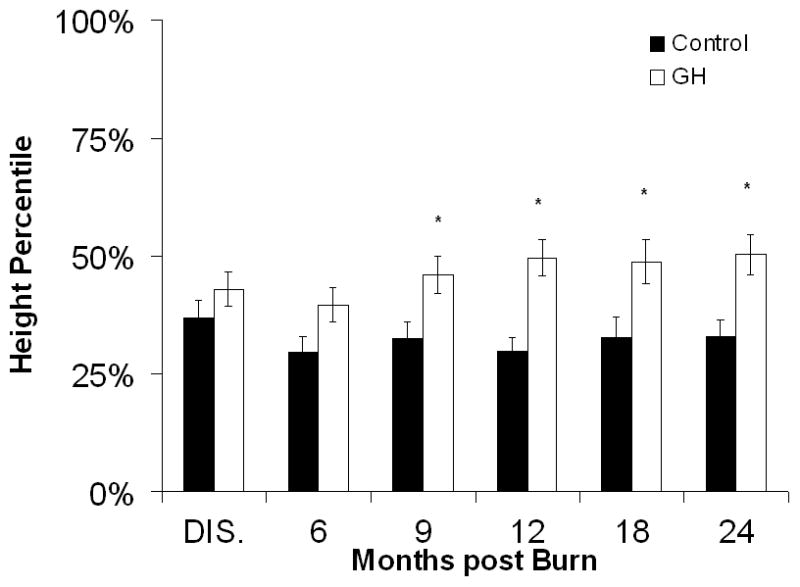
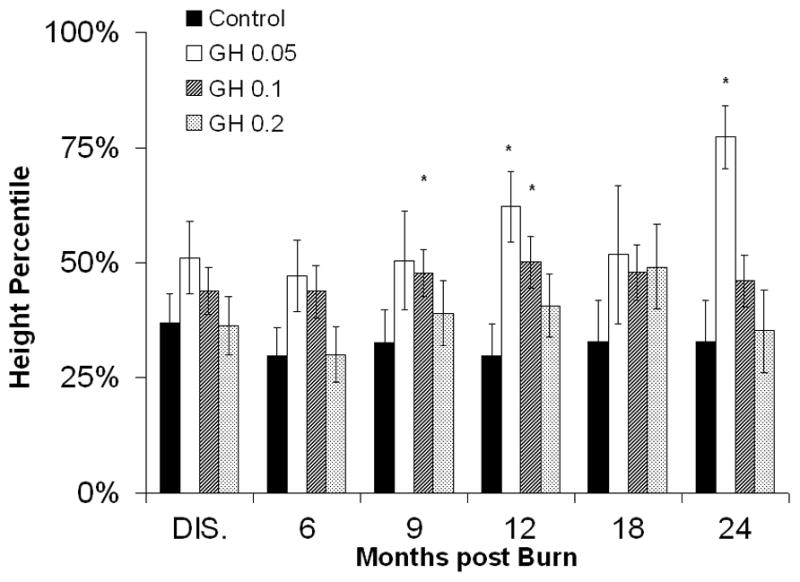
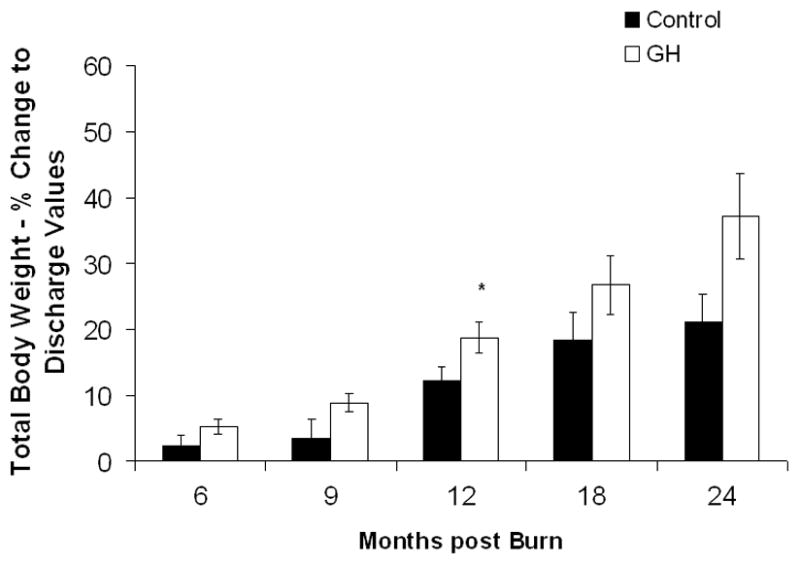
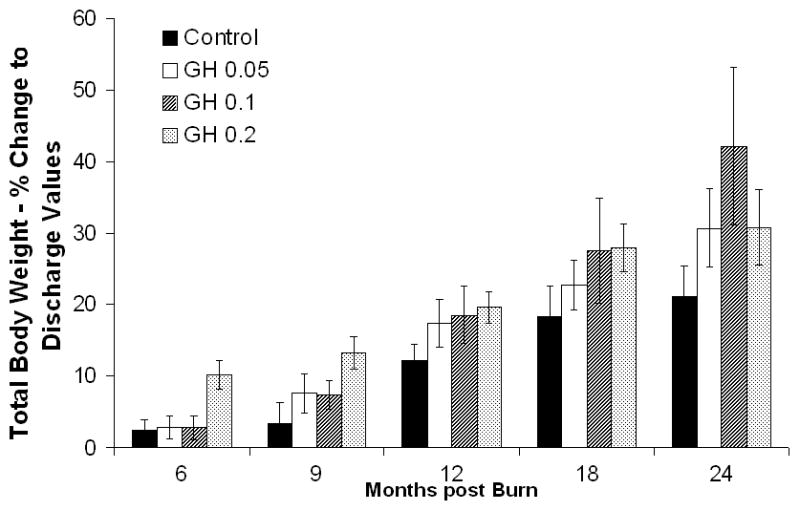
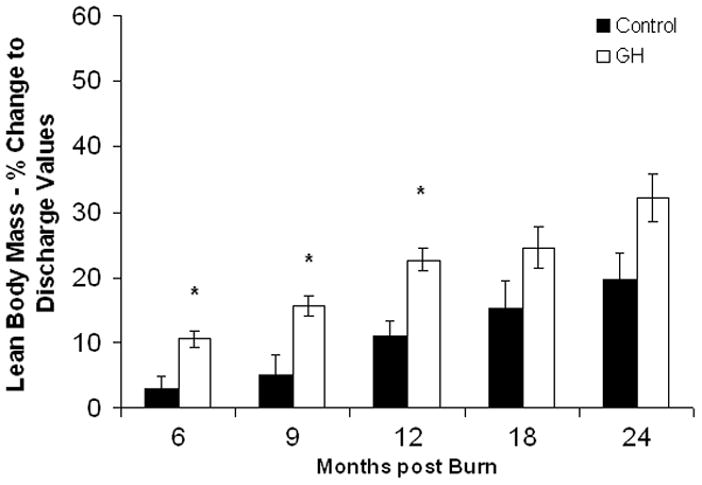
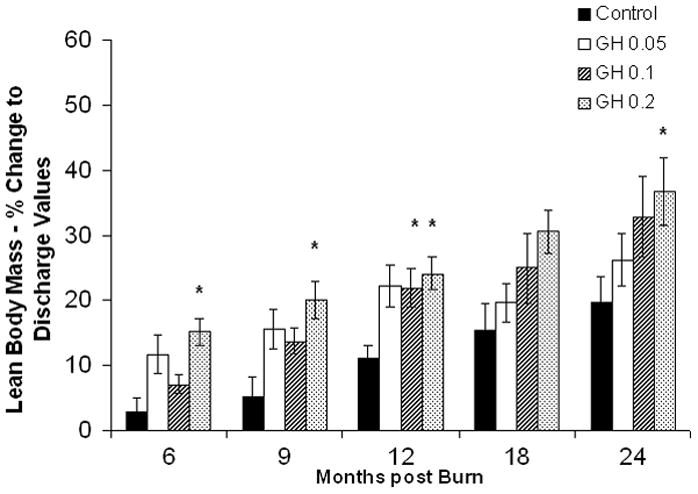
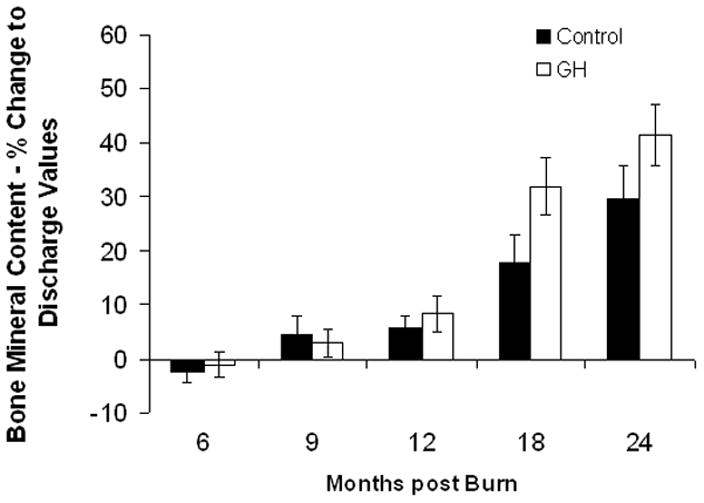
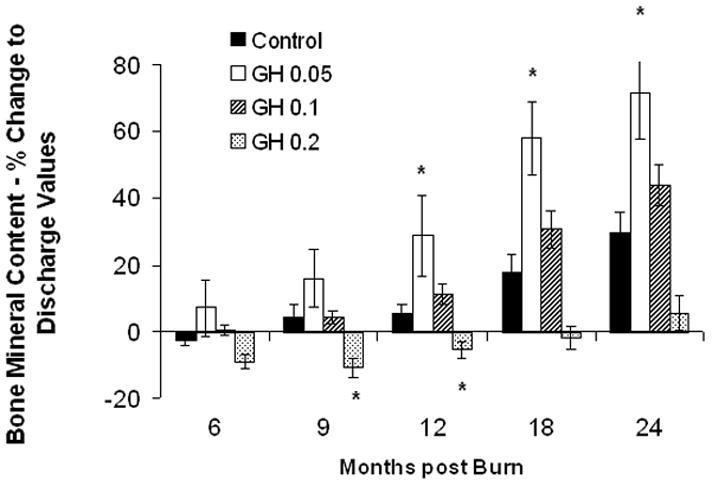
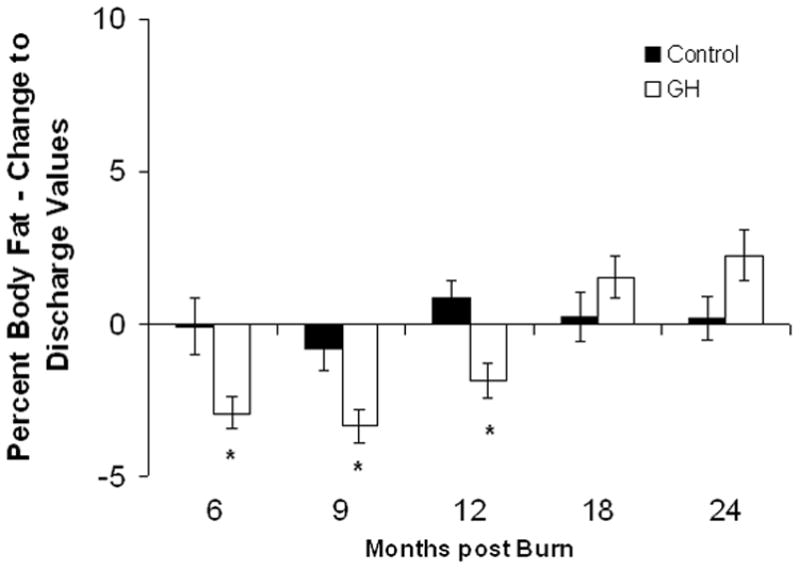
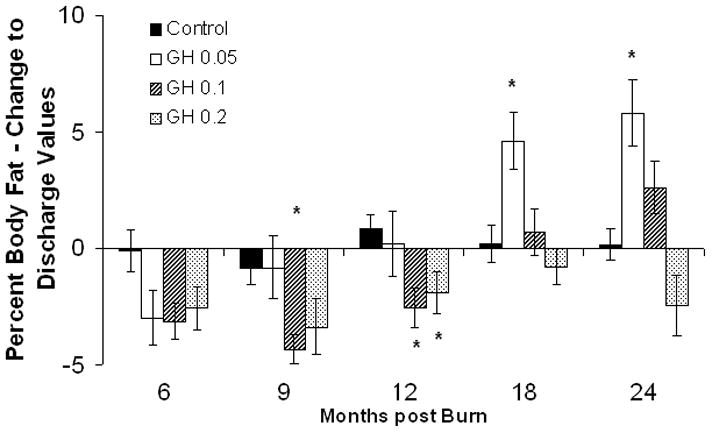
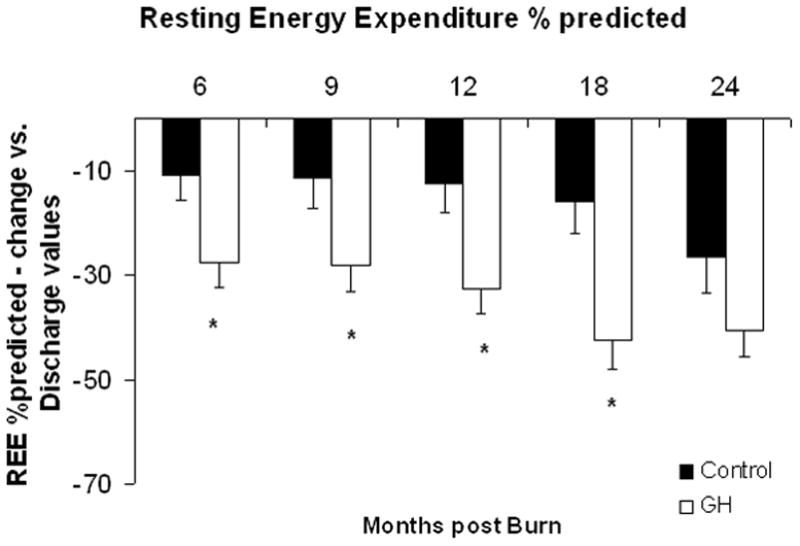
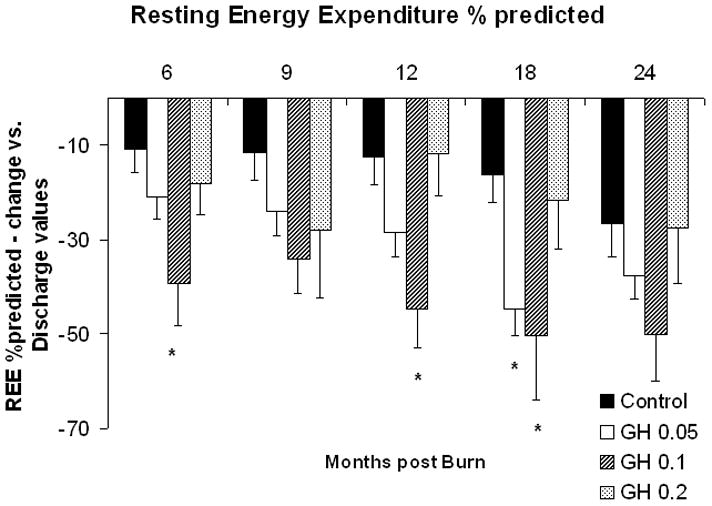
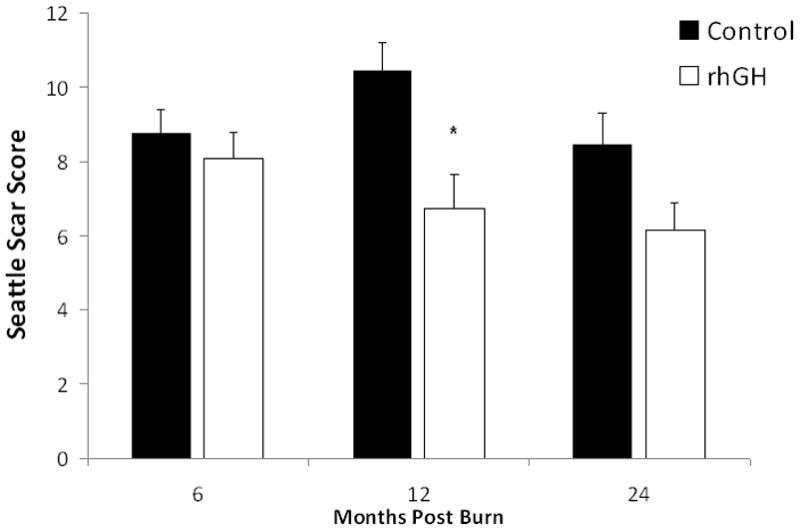
Results: RhGH administration markedly improved growth and lean body mass, whereas hypermetabolism was significantly attenuated. Serum growth hormone, insulin-like growth factor-I, and IGFBP-3 was significantly increased, whereas percent body fat content significantly decreased when compared with placebo, P < 0.05. A subset analysis revealed most lean body mass gain in the 0.2 mg/kg group, P < 0.05. Bone mineral content showed an unexpected decrease in the 0.2 mg/kg group, along with a decrease in PTH and increase in osteocalcin levels, P < 0.05. Resting energy expenditure improved with rhGH administration, most markedly in the 0.1 mg/kg/d rhGH group, P < 0.05. Cardiac output was decreased at 12 and 18 months postburn in the rhGH group. Long-term administration of 0.1 and 0.2 mg/kg/d rhGH significantly improved scarring at 12 months postburn, P < 0.05.
Conclusion: This large prospective clinical trial showed that long-term treatment with rhGH effectively enhances recovery of severely burned pediatric patients.
Figures
References
-
- Herndon DN, Tompkins RG. Support of the metabolic response to burninjury. Lancet. 2004;363:1895–1902. - PubMed
-
- Rutan RL, Herndon DN. Growth delay in postburn pediatric patients. Arch Surg. 1990;125:392–395. - PubMed
-
- Gore DC, Honeycutt D, Jahoor F, et al. Effect of exogenous growth hormone on glucose utilization in burn patients. J Surg Res. 1991;51:518–523. - PubMed
-
- Gore DC, Honeycutt D, Jahoor F, et al. Effect of exogenous growth hormone on whole-body and isolated-limb protein kinetics in burned patients. Arch Surg. 1991;126:38–43. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
