

Sex hormones and frailty in older men: the osteoporotic fractures in men (MrOS) study
- PMID: 19737923
- PMCID: PMC2758722
- DOI: 10.1210/jc.2009-0417
Sex hormones and frailty in older men: the osteoporotic fractures in men (MrOS) study
Abstract
Context: As men age, the prevalence of frailty increases whereas levels of androgens decline. Little is known about the relation between these factors.
Objective: The aim of this study was to assess cross-sectional and longitudinal associations of estradiol, bioavailable estradiol, testosterone, bioavailable testosterone (bioT), and SHBG with frailty status.
Design and setting: The Osteoporotic Fractures in Men (MrOS) study was conducted at six U.S. clinical centers.
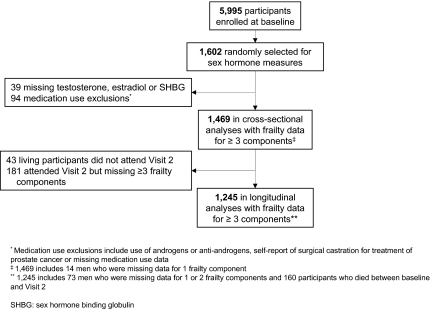
Participants: A total of 1469 community-dwelling men at least 65 yr old with baseline data participated; 1245 men had frailty status reassessed 4.1 yr later.
Main outcome measure: Proportional odds models estimated the likelihood of greater frailty status. Frail men had at least three of the following: weakness, slowness, low activity, exhaustion, and shrinking/sarcopenia; intermediate men had one or two criteria; and robust men had none. At follow-up, death was included as an additional ordinal outcome. Sex hormones were assayed by spectrometry/chromatographic methods.
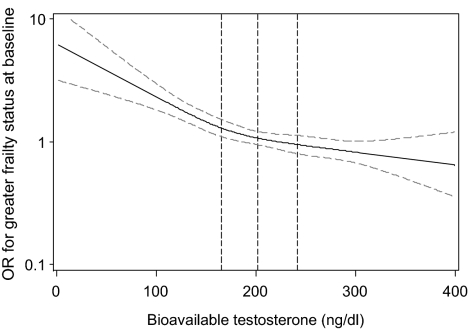
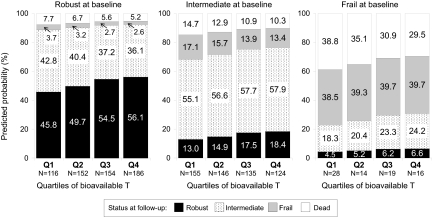
Results: In cross-sectional analyses, men in the lowest quartile of bioT had 1.39-fold (95% confidence interval, 1.02, 1.91) increased odds of greater frailty status compared to men in the highest quartile after adjustment for covariates including age, body size, health status, and medical conditions. In age-adjusted longitudinal analyses, men in the lowest quartile of bioT had 1.51-fold (95% confidence interval, 1.10, 2.07) increased odds of greater frailty status 4.1 yr later. This association was largely attenuated by adjustment for covariates. No other hormones were associated in a cross-sectional or longitudinal manner with frailty status after adjustment.
Conclusions: Low levels of bioT were independently associated with worse baseline frailty status. Frailty status should be considered as an outcome in trials of testosterone supplementation.
Figures
References
-
- Fried LP, Walston J 1998 Frailty and failure to thrive. In: Hazzard WR, Blass JP, Ettinger WHJ, Halter JB, Ouslander J, eds. Principles of geriatric medicine and gerontology. 4th ed. New York: McGraw Hill; 1387–1402
-
- Walston J, Hadley EC, Ferrucci L, Guralnik JM, Newman AB, Studenski SA, Ershler WB, Harris T, Fried LP 2006 Research agenda for frailty in older adults: toward a better understanding of physiology and etiology: summary from the American Geriatrics Society/National Institute on Aging Research Conference on Frailty in Older Adults. J Am Geriatr Soc 54:991–1001 - PubMed
-
- Fried LP, Tangen CM, Walston J, Newman AB, Hirsch C, Gottdiener J, Seeman T, Tracy R, Kop WJ, Burke G, McBurnie MA 2001 Frailty in older adults: evidence for a phenotype. J Gerontol A Biol Sci Med Sci 56:M146–156 - PubMed
-
- Bandeen-Roche K, Xue QL, Ferrucci L, Walston J, Guralnik JM, Chaves P, Zeger SL, Fried LP 2006 Phenotype of frailty: characterization in the women’s health and aging studies. J Gerontol A Biol Sci Med Sci 61:262–266 - PubMed
-
- Blaum CS, Xue QL, Michelon E, Semba RD, Fried LP 2005 The association between obesity and the frailty syndrome in older women: the Women’s Health and Aging Studies. J Am Geriatr Soc 53:927–934 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- U01 AR45654,/AR/NIAMS NIH HHS/United States
- K24 AR048841/AR/NIAMS NIH HHS/United States
- U01 AR45647/AR/NIAMS NIH HHS/United States
- U01 AR45614/AR/NIAMS NIH HHS/United States
- U01 AR045614/AR/NIAMS NIH HHS/United States
- U01 AR045654/AR/NIAMS NIH HHS/United States
- U01 AR045583/AR/NIAMS NIH HHS/United States
- U01 AG042140/AG/NIA NIH HHS/United States
- U01-AG027810,/AG/NIA NIH HHS/United States
- U01 AR45583/AR/NIAMS NIH HHS/United States
- U01 AG18197,/AG/NIA NIH HHS/United States
- U01 AR045647/AR/NIAMS NIH HHS/United States
- U01 AR45580/AR/NIAMS NIH HHS/United States
- U01 AG027810/AG/NIA NIH HHS/United States
- UL1 RR024140/RR/NCRR NIH HHS/United States
- U01 AR45632,/AR/NIAMS NIH HHS/United States
- U01 AR045580/AR/NIAMS NIH HHS/United States
- U01 AG018197/AG/NIA NIH HHS/United States
- U01 AR066160/AR/NIAMS NIH HHS/United States
- U01 AR045632/AR/NIAMS NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
