

Impact of venous thromboembolism and anticoagulation on cancer and cancer survival
- PMID: 19738120
- PMCID: PMC2799059
- DOI: 10.1200/JCO.2009.22.4584
Impact of venous thromboembolism and anticoagulation on cancer and cancer survival
Abstract
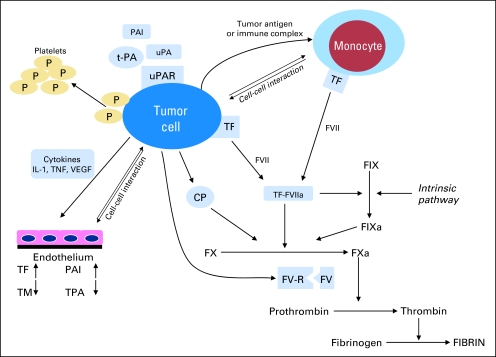
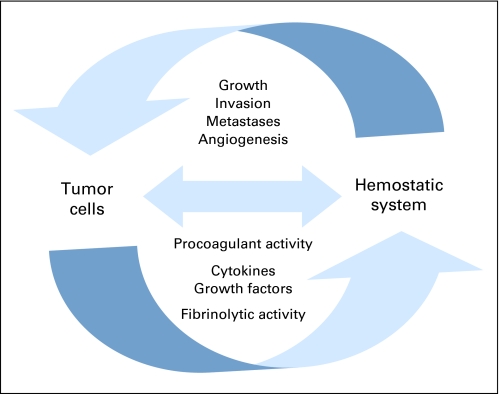
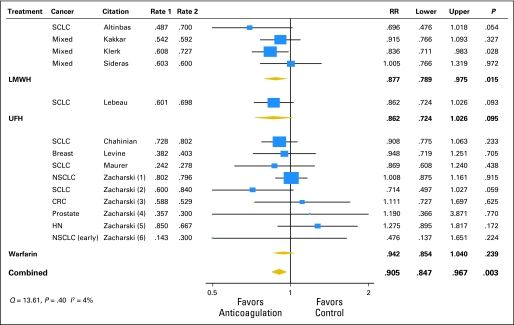
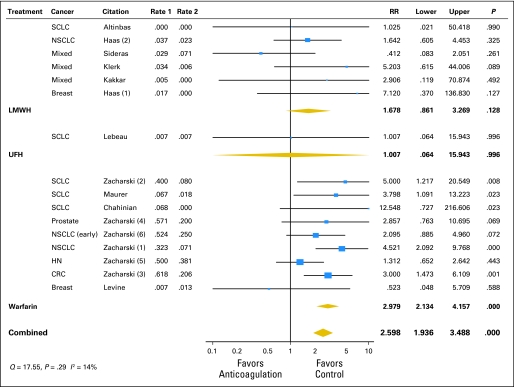
Changes in the hemostatic system and chronic hemostatic activation are frequently observed in patients with cancer, even in the absence of venous thromboembolism (VTE). VTE is a leading cause of death among patients with cancer and contributes to long-term mortality in patients with early as well as advanced-stage cancer. Mounting evidence suggests that components of the clotting cascade and associated vascular factors play an integral part in tumor progression, invasion, angiogenesis, and metastasis formation. Furthermore, there are intriguing in vitro and animal findings that anticoagulants, in particular the low molecular weight heparins (LMWHs), exert an antineoplastic effect through multiple mechanisms, including interference with tumor cell adhesion, invasion, metastasis formation, angiogenesis, and the immune system. Several relatively small randomized controlled clinical trials of anticoagulation as cancer therapy in patients without a VTE diagnosis have been completed. These comprise studies with LMWH, unfractionated heparin, and vitamin K antagonists, with overall encouraging but nonconclusive results and some limitations. Meta-analyses performed for the American Society of Clinical Oncology VTE Guidelines Committee and the Cochrane Collaboration suggest overall favorable effects of anticoagulation on survival of patients with cancer, mainly with LMWH. However, definitive clinical trials have been elusive and questions remain regarding the importance of tumor type and stage on treatment efficacy, the impact of fatal thromboembolic events, optimal anticoagulation therapy, and safety with differing chemotherapy regimens. Although the LMWHs and related agents hold promise for improving outcomes in patients with cancer, additional studies of their efficacy and safety in this setting are needed.
Conflict of interest statement
Authors' disclosures of potential conflicts of interest and author contributions are found at the end of this article.
Figures
References
-
- Heit JA, Silverstein MD, Mohr DN, et al. Risk factors for deep vein thrombosis and pulmonary embolism: A population-based case-control study. Arch Intern Med. 2000;160:809–815. - PubMed
-
- White R, Alcalay A, Zhou H, et al. Venous thromboembolism in 68,142 patients with colorectal cancer. J Thromb Haemost. 2005;3(suppl) abstr OR056.
-
- Green KB, Silverstein RL. Hypercoagulability in cancer. Hematol Oncol Clin North Am. 1996;10:499–530. - PubMed
-
- Rickles FR, Levine MN. Epidemiology of thrombosis in cancer. Acta Haematol. 2001;106:6–12. - PubMed
-
- Falanga A. Mechanisms of hypercoagulation in malignancy and during chemotherapy. Haemostasis. 1998;28(suppl 3):50–60. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
