

On the effectiveness of care co-ordination services aimed at preventing hospital admissions and emergency attendances
- PMID: 19739360
- PMCID: PMC2713026
- DOI: 10.1007/s10729-008-9092-5
On the effectiveness of care co-ordination services aimed at preventing hospital admissions and emergency attendances
Abstract
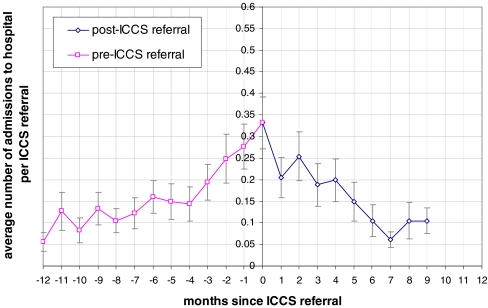
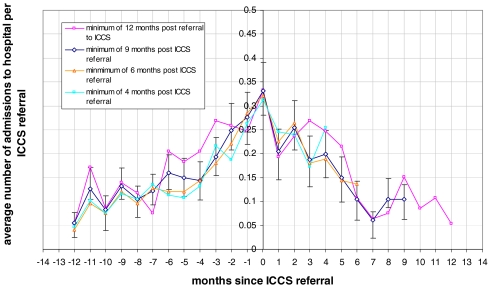
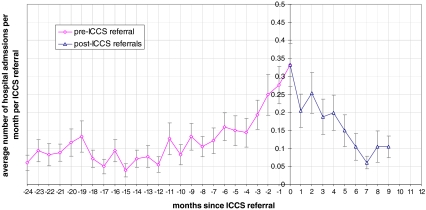
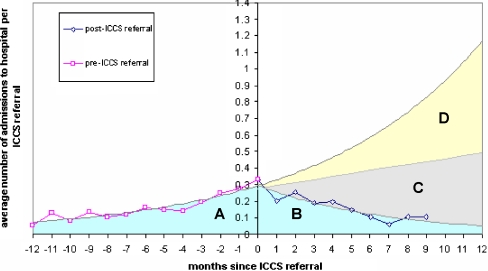
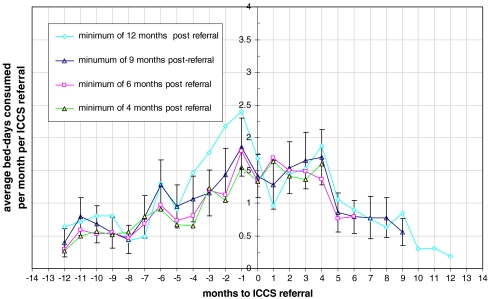
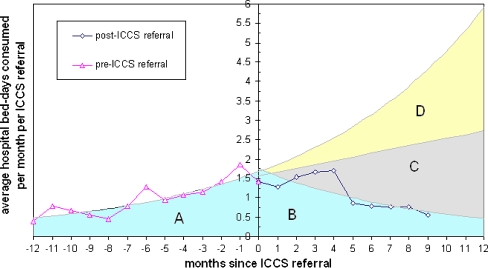
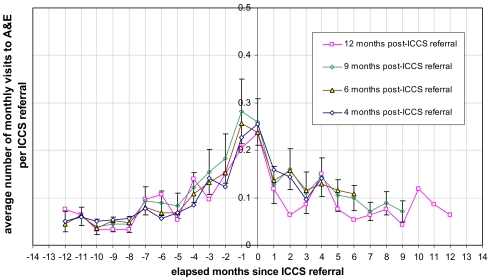
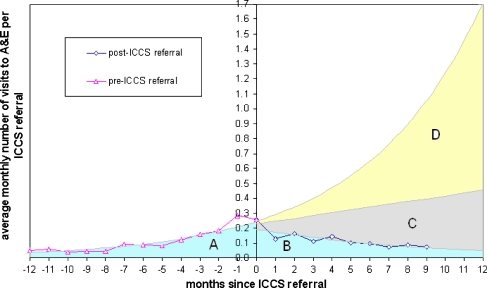
Finding alternatives to hospital admissions for older people and helping them to live for as long as possible in their own homes is a key objective of UK health and social policy. However, there is a lack of proof as to whether such alternatives actually work and are cost-effective. The research reported in this paper is based on an evaluation of a care co-ordination service with the aim helping people to remain at home and preventing unnecessary hospital admissions and A&E attendances. An initial evaluation found that the effectiveness of the service was at best marginal. The new method of evaluation described in this paper tracks patient attendance at A&E departments and hospital stays 12 months before they are accepted into the care co-ordination service and evaluates the resultant savings in health care activity. It finds that the service results in between 14 and 29 saved hospital bed days per client per year and between three and eight A&E attendances. Whilst the service does not arrest functional decline in individuals, the incidence of falls is significantly reduced, and that the effect on quality of life is neutral to broadly favourable. It finds that mortality levels are higher than in the general population of similar age but this is probably due to selection effects because clients are unhealthier from the outset, and that in the 90+ age group there is no significant difference. Without the benefit of a control group it is not possible to confirm the results with certainty, but corroborating independent evidence is provided that supports the conclusions reached.
Figures
Similar articles
-
The impact of a new emergency admission avoidance system for older people on length of stay and same-day discharges.Age Ageing. 2014 Jan;43(1):116-21. doi: 10.1093/ageing/aft086. Epub 2013 Aug 1. Age Ageing. 2014. PMID: 23907007
-
What are the Costs and Benefits of Providing Comprehensive Seven-day Services for Emergency Hospital Admissions?Health Econ. 2015 Aug;24(8):907-12. doi: 10.1002/hec.3207. Epub 2015 May 22. Health Econ. 2015. PMID: 26010243
-
Emergency hospital care for adults with suspected seizures in the NHS in England 2007-2013: a cross-sectional study.BMJ Open. 2018 Oct 21;8(10):e023352. doi: 10.1136/bmjopen-2018-023352. BMJ Open. 2018. PMID: 30344177 Free PMC article.
-
Cost reduction strategies for emergency services: insurance role, practice changes and patients accountability.Health Care Anal. 2009 Mar;17(1):1-19. doi: 10.1007/s10728-008-0081-0. Epub 2008 Feb 28. Health Care Anal. 2009. PMID: 18306043 Review.
-
Systematic reviews of the effectiveness of day care for people with severe mental disorders: (1) acute day hospital versus admission; (2) vocational rehabilitation; (3) day hospital versus outpatient care.Health Technol Assess. 2001;5(21):1-75. doi: 10.3310/hta5210. Health Technol Assess. 2001. PMID: 11532238 Review.
Cited by
-
Comprehensive Cardiac Care: How Much Does It Cost?Int J Environ Res Public Health. 2023 Mar 11;20(6):4980. doi: 10.3390/ijerph20064980. Int J Environ Res Public Health. 2023. PMID: 36981889 Free PMC article.
-
The role of matched controls in building an evidence base for hospital-avoidance schemes: a retrospective evaluation.Health Serv Res. 2012 Aug;47(4):1679-98. doi: 10.1111/j.1475-6773.2011.01367.x. Epub 2012 Jan 6. Health Serv Res. 2012. PMID: 22224902 Free PMC article.
-
Measuring the impact of an acute visiting scheme on emergency department attendances - a pre-post cohort design.BMC Health Serv Res. 2021 May 28;21(1):521. doi: 10.1186/s12913-021-06557-3. BMC Health Serv Res. 2021. PMID: 34049540 Free PMC article.
-
Evaluating the impact of healthcare interventions using routine data.BMJ. 2019 Jun 20;365:l2239. doi: 10.1136/bmj.l2239. BMJ. 2019. PMID: 31221675 Free PMC article. No abstract available.
-
Interventions to Prevent Potentially Avoidable Hospitalizations: A Mixed Methods Systematic Review.Front Public Health. 2022 Jul 11;10:898359. doi: 10.3389/fpubh.2022.898359. eCollection 2022. Front Public Health. 2022. PMID: 35899150 Free PMC article.
References
-
- None
- Alder (2008) Disease Management programmes for major depression: Making the financial case. Milliman Research Report, Milliman, London
-
- Bowen T, Forte P (2000) Intermediate Care Services for Older People: Estimating Future Workforce Requirements, Unpublished report
-
- {'text': '', 'ref_index': 1, 'ids': [{'type': 'DOI', 'value': '10.1111/j.1467-842X.2000.tb00131.x', 'is_inner': False, 'url': 'https://doi.org/10.1111/j.1467-842x.2000.tb00131.x'}, {'type': 'PubMed', 'value': '10790930', 'is_inner': True, 'url': 'https://pubmed.ncbi.nlm.nih.gov/10790930/'}]}
- Byles JE (2000) A thorough going over: evidence for health assessments for older persons. Aust N Z J Public Health 24(2):117–123 - PubMed
-
- Brent Council (2007) Brent partnerships for older people project—12 months on. May 2007, Internal report.
-
- Campbell DT, Stanley JC (1966) Experimental and quasi-experimental designs for research. Reprinted from Handbook of Research on Teaching, published in 1963 by Houghton Mifflin Company.
MeSH terms
LinkOut - more resources
Full Text Sources