

Detection of macular ganglion cell loss in glaucoma by Fourier-domain optical coherence tomography
- PMID: 19744726
- PMCID: PMC2787911
- DOI: 10.1016/j.ophtha.2009.05.025
Detection of macular ganglion cell loss in glaucoma by Fourier-domain optical coherence tomography
Abstract
Purpose: To map ganglion cell complex (GCC) thickness with high-speed Fourier-domain optical coherence tomography (FD-OCT) and compute novel macular parameters for glaucoma diagnosis.
Design: Observational, cross-sectional study.
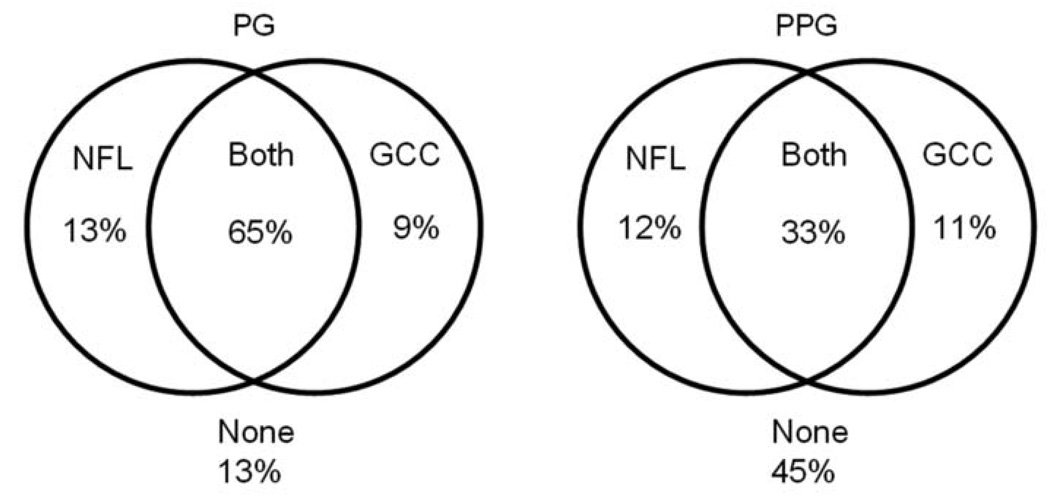
Participants: One hundred seventy-eight participants in the Advanced Imaging for Glaucoma Study, divided into 3 groups: 65 persons in the normal group, 78 in the perimetric glaucoma group (PG), and 52 in the preperimetric glaucoma group (PPG).
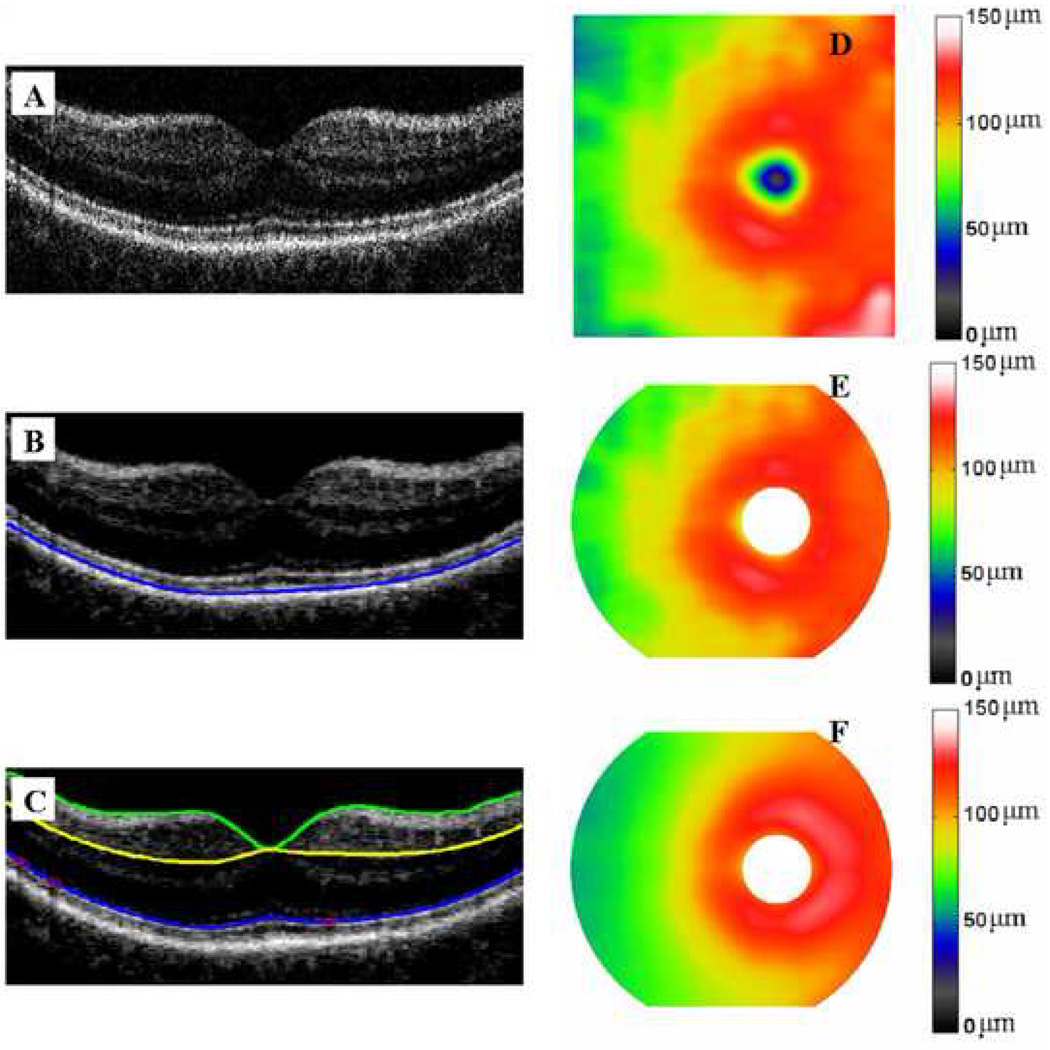
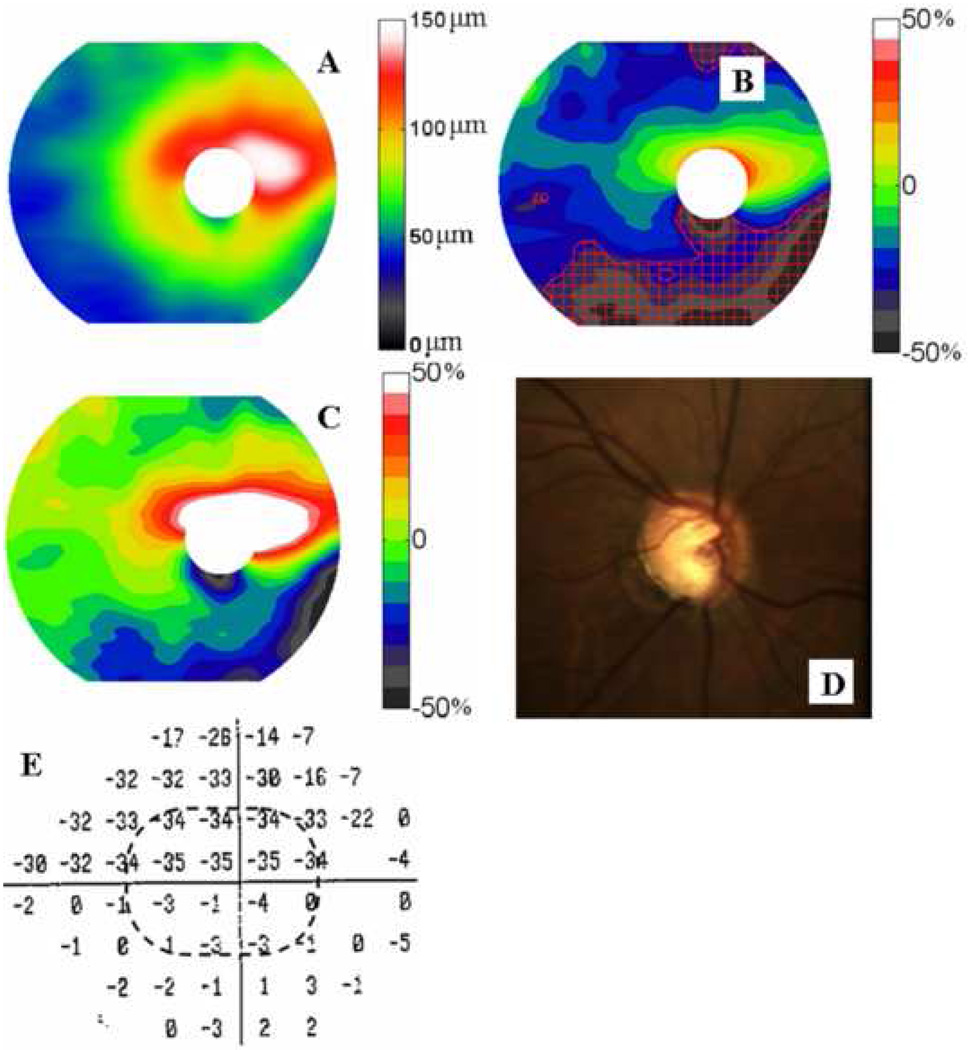
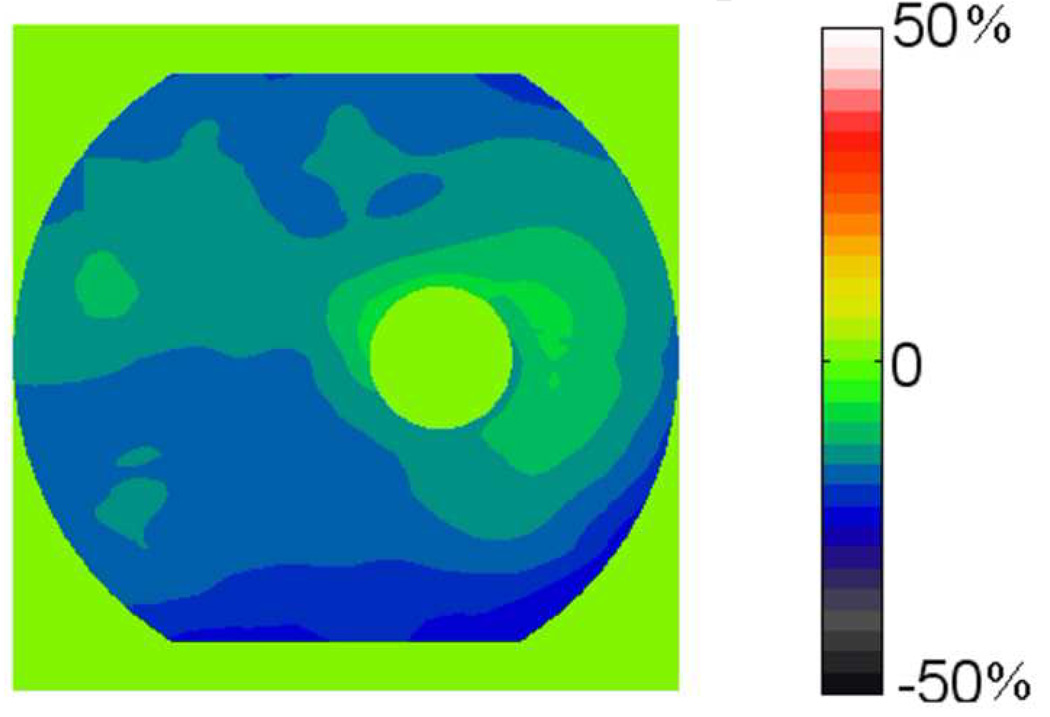
Methods: The RTVue FD-OCT system was used to map the macula over a 7 x 6 mm region. The macular OCT images were exported for automatic segmentation using software we developed. The program measured macular retinal (MR) thickness and GCC thickness. The GCC was defined as the combination of nerve fiber, ganglion cell, and inner plexiform layers. Pattern analysis was applied to the GCC map and the diagnostic powers of pattern-based diagnostic parameters were investigated. Results were compared with time-domain (TD) Stratus OCT measurements of MR and circumpapillary nerve fiber layer (NFL) thickness.
Main outcome measures: Repeatability was assessed by intraclass correlation, pooled standard deviation, and coefficient of variation. Diagnostic power was assessed by the area under the receiver operator characteristic (AROC) curve. Measurements in the PG group were the primary measures of performance.
Results: The FD-OCT measurements of MR and GCC averages had significantly better repeatability than TD-OCT measurements of MR and NFL averages. The FD-OCT GCC average had significantly (P = 0.02) higher diagnostic power (AROC = 0.90) than MR (AROC = 0.85 for both FD-OCT and TD-OCT) in differentiating between PG and normal. One GCC pattern parameter, global loss volume, had significantly higher AROC (0.92) than the overall average (P = 0.01). The diagnostic powers of the best GCC parameters were statistically equal to TD-OCT NFL average.
Conclusions: The higher speed and resolution of FD-OCT improved the repeatability of macular imaging compared with standard TD-OCT. Ganglion cell mapping and pattern analysis improved diagnostic power. The improved diagnostic power of macular GCC imaging is on par with, and complementary to, peripapillary NFL imaging. Macular imaging with FD-OCT is a useful method for glaucoma diagnosis and has potential for tracking glaucoma progression.
Figures



References
-
- Quigley HA, Dunkelberger GR, Green WR. Retinal ganglion cell atrophy correlated with automated perimetry in human eyes with glaucoma. Am J Ophthalmol. 1989;107:453–464. - PubMed
-
- Quigley HA, Miller NR, George T. Clinical evaluation of nerve fiber layer atrophy as an indicator of glaucomatous optic nerve damage. Arch Ophthalmol. 1980;98:1564–1571. - PubMed
-
- Sommer A, Miller NR, Pollack I, et al. The nerve fiber layer in the diagnosis of glaucoma. Arch Ophthalmol. 1977;95:2149–2156. - PubMed
-
- Sommer A, Quigley HA, Robin AL, et al. Evaluation of nerve fiber layer assessment. Arch Ophthalmol. 1984;102:1766–1771. - PubMed
-
- Pederson JE, Anderson DR. The mode of progressive disc cupping in ocular hypertension and glaucoma. Arch Ophthalmol. 1980;98:490–495. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
