

Pulmonary perfusion heterogeneity is increased by sustained, heavy exercise in humans
- PMID: 19745192
- PMCID: PMC2777793
- DOI: 10.1152/japplphysiol.00491.2009
Pulmonary perfusion heterogeneity is increased by sustained, heavy exercise in humans
Abstract
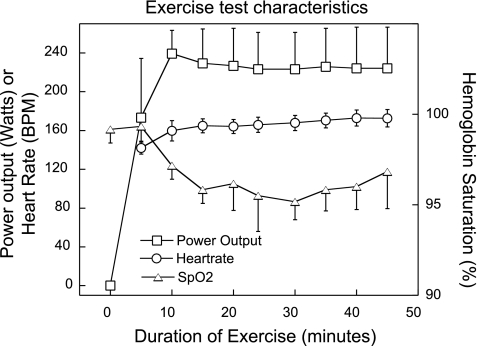
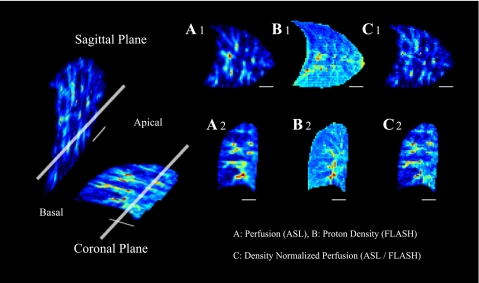
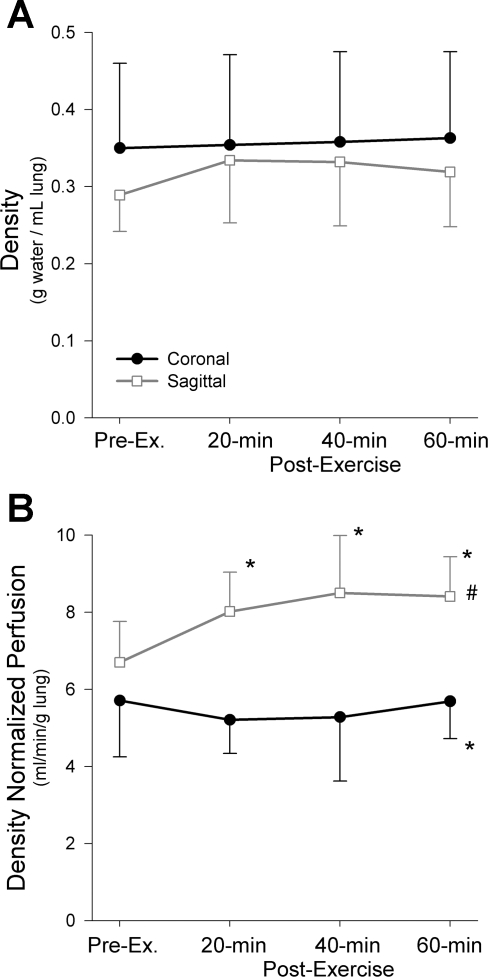
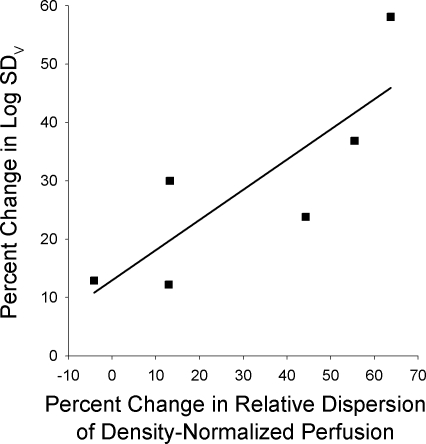
Exercise presents a considerable stress to the pulmonary system and ventilation-perfusion (Va/Q) heterogeneity increases with exercise, affecting the efficiency of gas exchange. In particular, prolonged heavy exercise and maximal exercise are known to increase Va/Q heterogeneity and these changes persist into recovery. We hypothesized that the spatial heterogeneity of pulmonary perfusion would be similarly elevated after prolonged exercise. To test this, athletic subjects (n = 6, Vo(2max) = 61 ml. kg(-1).min(-1)) with exercising Va/Q heterogeneity previously characterized by the multiple inert gas elimination technique (MIGET), performed 45 min of cycle exercise at approximately 70% Vo(2max). MRI arterial spin labeling measures of pulmonary perfusion were acquired pre- and postexercise (at 20, 40, 60 min post) to quantify the spatial distribution in isogravitational (coronal) and gravitationally dependent (sagittal) planes. Regional proton density measurements allowed perfusion to be normalized for density and quantified in milliliters per minute per gram. Mean lung density did not change significantly in either plane after exercise (P = 0.19). Density-normalized perfusion increased in the sagittal plane postexercise (P =or <0.01) but heterogeneity did not (all P >or= 0.18), likely because of perfusion redistribution and vascular recruitment. Density-normalized perfusion was unchanged in the coronal plane postexercise (P = 0.66), however, perfusion heterogeneity was significantly increased as measured by the relative dispersion [RD, pre 0.62(0.07), post 0.82(0.21), P < 0.0001] and geometric standard deviation [GSD, pre 1.74(0.14), post 2.30(0.56), P < 0.005]. These changes in heterogeneity were related to the exercise-induced changes of the log standard deviation of the ventilation distribution, an MIGET index of Va/Q heterogeneity (RD R(2) = 0.68, P < 0.05, GSD, R(2) = 0.55, P = 0.09). These data are consistent with but not proof of interstitial pulmonary edema as the mechanism underlying exercise-induced increases in both spatial perfusion heterogeneity and Va/Q heterogeneity.
Figures

References
-
- Anholm JD, Milne EN, Stark P, Bourne JC, Friedman P. Radiographic evidence of interstitial pulmonary edema after exercise at altitude. J Appl Physiol 86: 503–509, 1999. - PubMed
-
- Beaver WL, Wasserman K, Whipp BJ. A new method for detecting anaerobic threshold by gas exchange. J Appl Physiol 60: 2020–2027, 1986. - PubMed
-
- Bernard SL, Glenny RW, Erickson HH, Fedde MR, Polissar N, Basaraba RJ, Hlastala MP. Minimal redistribution of pulmonary blood flow with exercise in racehorses. J Appl Physiol 81: 1062–1070, 1996. - PubMed
-
- Bolar DS, Levin DL, Hopkins SR, Frank LF, Liu TT, Wong EC, Buxton RB. Quantification of regional pulmonary blood flow using ASL-FAIRER. Magn Reson Med 55: 1308, 2006. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous