

HIV infection does not affect active case finding of tuberculosis in South African gold miners
- PMID: 19745207
- PMCID: PMC2796737
- DOI: 10.1164/rccm.200806-846OC
HIV infection does not affect active case finding of tuberculosis in South African gold miners
Abstract
Rationale: Gold miners in South Africa undergo annual radiological screening for tuberculosis in an occupational health center of a gold mining company, but the optimal screening algorithm is unclear.
Objectives: To evaluate methods for active case detection of tuberculosis.
Methods: A sequential sample of miners attending annual medical examination was screened for tuberculosis using a symptom questionnaire, chest radiograph, and two sputum specimens for microscopy and culture.
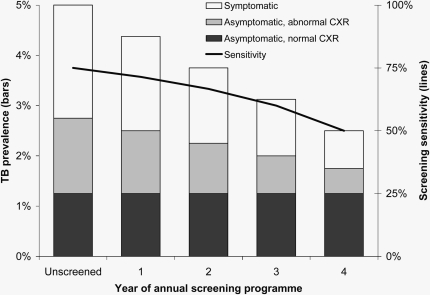
Measurements and main results: There were 1,955 miners included in this study; all were male with a median age of 41 years (range, 20-61 yr). Presence of at least one of a trio of symptoms (new or worsening cough, night sweats, or weight loss) had similar sensitivity (29.4%) to either chest radiograph (25.5%) or sputum smear (25.5%). These sensitivities did not differ by HIV status. Presence of one or more elements of the symptom trio and/or new radiological abnormality substantially increased sensitivity to 49.0%. Specificity of the symptom trio was higher in HIV-uninfected (91.8%) than in HIV-infected persons (88.2%; P = 0.018). Specificity of chest radiography and smear were similar (98.7% and 99.0%, respectively) and did not differ by HIV status (both P values > 0.8).
Conclusions: In a population of gold miners who undergo regular radiological screening, the addition of chest radiography to symptom screening substantially improved the sensitivity and positive predictive value. HIV infection did not alter the sensitivity of the screening tool.
Figures
Comment in
-
Sorting out icebergs, mirages, and clinical tuberculosis during active case finding.Am J Respir Crit Care Med. 2009 Dec 15;180(12):1167-9. doi: 10.1164/rccm.200909-1332ED. Am J Respir Crit Care Med. 2009. PMID: 19949239 No abstract available.
References
-
- Corbett EL, Marston B, Churchyard GJ, De Cock KM. Tuberculosis in sub-Saharan Africa: opportunities, challenges, and change in the era of antiretroviral treatment. Lancet 2006;367:926–937. - PubMed
-
- Nyunt UT, Ko Gyi U, Kahn G, Than Tin D, Aye UB. Tuberculosis baseline survey in Burma in 1972. Tubercle 1974;55:313–325. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
