

Impact of high-dose chemotherapy on the ability to deliver subsequent local-regional radiotherapy for breast cancer: analysis of Cancer and Leukemia Group B Protocol 9082
- PMID: 19747781
- PMCID: PMC3670136
- DOI: 10.1016/j.ijrobp.2009.04.013
Impact of high-dose chemotherapy on the ability to deliver subsequent local-regional radiotherapy for breast cancer: analysis of Cancer and Leukemia Group B Protocol 9082
Abstract
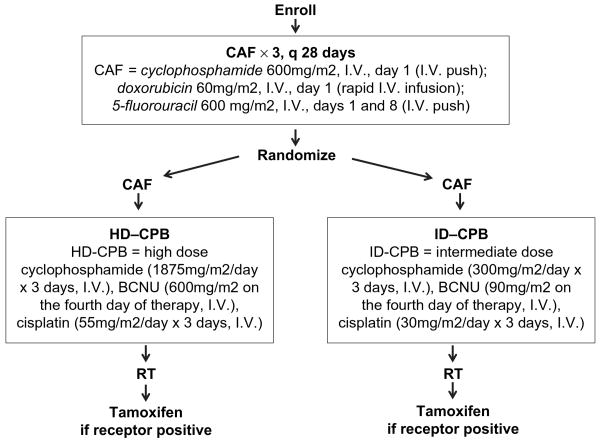
Purpose: To report, from Cancer and Leukemia Group B Protocol 9082, the impact of high-dose cyclophosphamide, cisplatin, and BCNU (HD-CPB) vs. intermediate-dose CPB (ID-CPB) on the ability to start and complete the planned course of local-regional radiotherapy (RT) for women with breast cancer involving >or=10 axillary nodes.
Methods and materials: From 1991 to 1998, 785 patients were randomized. The HD-CPB and ID-CPB arms were balanced regarding patient characteristics. The HD-CPB and ID-CPB arms were compared on the probability of RT initiation, interruption, modification, or incompleteness. The impact of clinical variables and interactions between variables were also assessed.
Results: Radiotherapy was initiated in 82% (325 of 394) of HD-CPB vs. 92% (360 of 391) of ID-CPB patients (p = 0.001). On multivariate analyses, RT was less likely given to patients who were randomized to HD treatment (odds ratio [OR] = 0 .38, p < 0.001), older (p = 0.005), African American (p = 0.003), postmastectomy (p = 0.02), or estrogen receptor positive (p = 0.03). High-dose treatment had a higher rate of RT interruption (21% vs. 12%, p = 0.001, OR = 2.05), modification (29% vs. 14%, p = 0.001, OR = 2.46), and early termination of RT (9% vs. 2%, p = 0.0001, OR = 5.35), compared with ID.
Conclusion: Treatment arm significantly related to initiation, interruption, modification, and early termination of RT. Patients randomized to HD-CPB were less likely to initiate RT, and of those who did, they were more likely to have RT interrupted, modified, and terminated earlier than those randomized to ID-CPB. The observed lower incidence of RT usage in African Americans vs. non-African Americans warrants further study.
Conflict of interest statement
Conflict of interest: L.B.M. receives honoraria from Varian Medical Systems, and grants from the National Institutes of Health, the Lance Armstrong Foundation, and the U.S. Department of Defense. P.G.R. receives an honorarium from Millennium Pharmaceuticals.
Figures
References
-
- Jones SE, Moon TE, Bonadonna G, et al. Comparison of different trials of adjuvant chemotherapy in stage II breast cancer using a natural history database. Am J Clin Oncol. 1987;10:387–395. - PubMed
-
- Hellman S, Harris JR. Natural history of breast cancer. In: Harris JR, Lippman ME, Morrow M, editors. Diseases of the breast. 2nd. Philadelphia: Lippincott Williams & Wilkins; 2000. pp. 407–424.
-
- Hoehne F, Chen S, Mabry H, et al. An update on prognosis in breast cancer patients with extensive axillary disease. Breast J. 2008;14:76–80. - PubMed
-
- Rack B, Janni W, Gerber B, et al. Patients with recurrent breast cancer: Does the primary axillary lymph node status predict more aggressive tumor progression? Breast Cancer Res Treat. 2003;82:83–92. - PubMed
-
- Montero AJ, Rouzier R, Lluch A, et al. The natural history of breast carcinoma in patients with ≥10 metastatic axillary lymph nodes before and after the advent of adjuvant therapy: A multi-institutional retrospective study. Cancer. 2005;104:229–235. - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
Grants and funding
- CA33601/CA/NCI NIH HHS/United States
- CA11789/CA/NCI NIH HHS/United States
- U10 CA029511/CA/NCI NIH HHS/United States
- CA47577/CA/NCI NIH HHS/United States
- CA32291/CA/NCI NIH HHS/United States
- U10 CA033601/CA/NCI NIH HHS/United States
- CA60138/CA/NCI NIH HHS/United States
- CA35279/CA/NCI NIH HHS/United States
- CA14028/CA/NCI NIH HHS/United States
- U10 CA077651/CA/NCI NIH HHS/United States
- CA77202/CA/NCI NIH HHS/United States
- U10 CA042777/CA/NCI NIH HHS/United States
- CA42777/CA/NCI NIH HHS/United States
- U10 CA047577/CA/NCI NIH HHS/United States
- U10 CA032291/CA/NCI NIH HHS/United States
- U10 CA035279/CA/NCI NIH HHS/United States
- U10 CA077202/CA/NCI NIH HHS/United States
- CA03927/CA/NCI NIH HHS/United States
- U10 CA031946/CA/NCI NIH HHS/United States
- CA77651/CA/NCI NIH HHS/United States
- U10 CA014028/CA/NCI NIH HHS/United States
- CA29511/CA/NCI NIH HHS/United States
- CA31946/CA/NCI NIH HHS/United States
- U10 CA003927/CA/NCI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
