

Loop diuretics in acute decompensated heart failure: necessary? Evil? A necessary evil?
- PMID: 19750134
- PMCID: PMC2742422
- DOI: 10.1161/CIRCHEARTFAILURE.108.821785
Loop diuretics in acute decompensated heart failure: necessary? Evil? A necessary evil?
Abstract
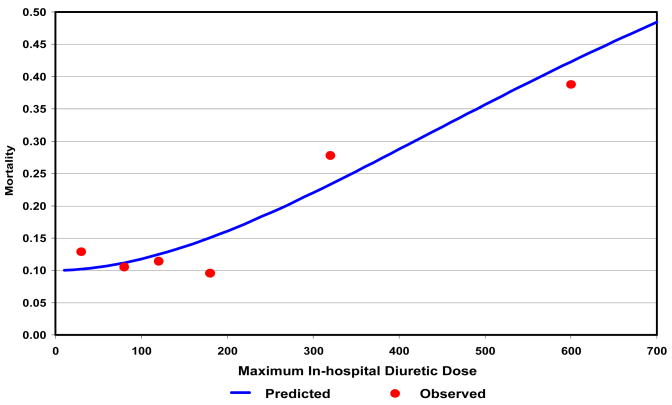
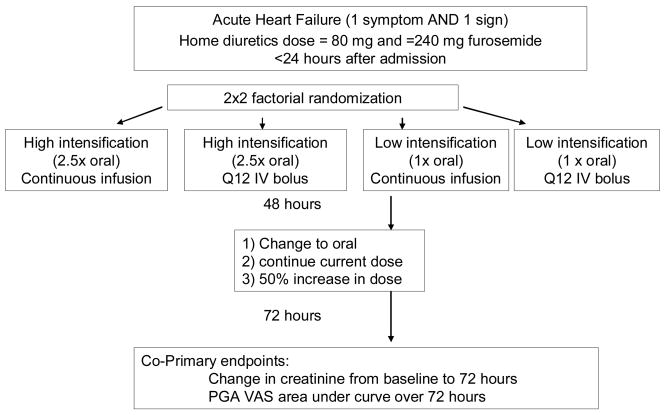
Acute decompensated heart failure (ADHF) is a common and highly morbid cardiovascular disorder. Most hospitalizations for ADHF are related to symptoms of congestion, and the vast majority of ADHF patients are treated with intravenous loop diuretics. Despite this nearly ubiquitous use, data supporting the safety and efficacy of loop diuretics in ADHF are limited, and controversy exists about the best way to use loop diuretics with regard to both dosing and means of administration (continuous infusion vs. intermittent boluses). We reviewed the data supporting the safety and efficacy of loop diuretics in patients with ADHF. A large body of observational literature suggests that loop diuretics, especially at higher doses, may be associated with increased mortality in patients with heart failure even after detailed adjustment for other measures of disease severity. Additionally, multiple small underpowered trials suggest that continuous infusion may be equivalent or superior to intermittent bolus dosing. In summary, there is a critical need to develop more robust data on the use of loop diuretics in ADHF. In that context, the NIH Heart Failure Clinical Research Network has begun the Diuretics Optimization Strategies Evaluation (DOSE) study, a multi-center, double-blind, randomized controlled trial that will enroll 300 patients with ADHF. The DOSE study will randomize patients using a 2 × 2 factorial design to low dose vs. high dose furosemide, and intermittent bolus vs. continuous infusion. Successful completion of the DOSE study will provide important data on the optimal clinical use of loop diuretics in ADHF.
Keywords: acute decompensated heart failure; clinical trials; diuretics.
Conflict of interest statement
Figures
References
-
-
Members of the Statistics C, Stroke Statistics S, Thom T, Haase N, Rosamond W, Howard VJ, Rumsfeld J, Manolio T, Zheng ZJ, Flegal K, O’Donnell C, Kittner S, Lloyd-Jones D, Goff DC, Jr, Hong Y, Adams R, Friday G, Furie K, Gorelick P, Kissela B, Marler J, Meigs J, Roger V, Sidney S, Sorlie P, Steinberger J, Wasserthiel-Smoller S, Wilson M, Wolf P. Heart Disease and Stroke Statistics--2006 Update: A Report From the American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Circulation. 2006;113:e85–151.
-
-
- Felker GM, Adams KF, Konstam MA, O’Connor CM, Gheorghiade M. The problem of decompensated heart failure: Nomenclature, classification, and risk stratification. Am Heart J. 2003;145:S18–S25. - PubMed
-
- Felker GM, Leimberger JD, Califf RM, Cuffe MS, Massie BM, Adams KF, Jr, Gheorghiade M, O’Connor CM. Risk stratification after hospitalization for decompensated heart failure. J Card Fail. 2004;10:460–466. - PubMed
-
- Lee DS, Austin PC, Rouleau JL, Liu PP, Naimark D, Tu JV. Predicting Mortality Among Patients Hospitalized for Heart Failure: Derivation and Validation of a Clinical Model. JAMA: The Journal of the American Medical Association. 2003;290:2581–2587. - PubMed
-
- Ramirez A, Abelmann WH. Cardiac decompensation. New Eng J Med. 1974;290:499–501. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
