

Advances in diagnosis, treatment and palliation of cholangiocarcinoma: 1990-2009
- PMID: 19750567
- PMCID: PMC2744180
- DOI: 10.3748/wjg.15.4240
Advances in diagnosis, treatment and palliation of cholangiocarcinoma: 1990-2009
Abstract
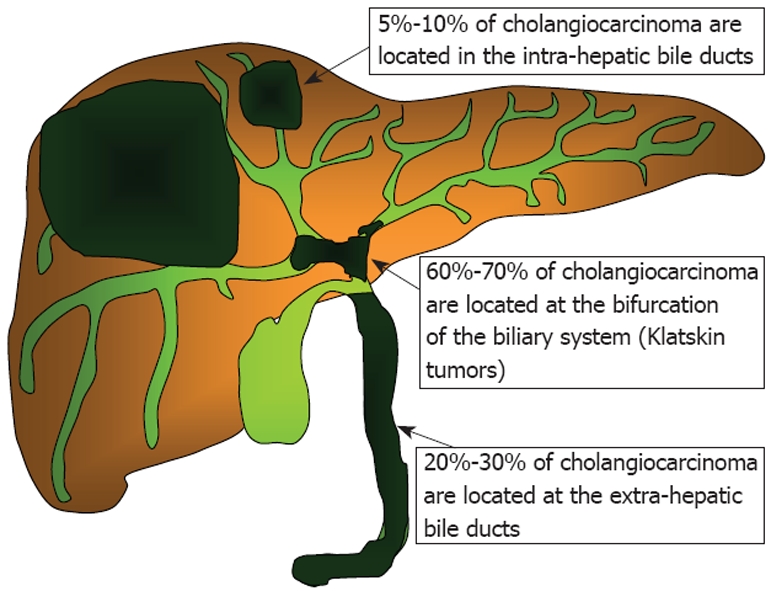
Several advances in diagnosis, treatment and palliation of cholangiocarcinoma (CC) have occurred in the last decades. A multidisciplinary approach to this disease is therefore recommended. CC is a relatively rare tumor and the main risk factors are: chronic inflammation, genetic predisposition and congenital abnormalities of the biliary tree. While the incidence of intra-hepatic CC is increasing, the incidence of extra-hepatic CC is trending down. The only curative treatment for CC is surgical resection with negative margins. Liver transplantation has been proposed only for selected patients with hilar CC that cannot be resected who have no metastatic disease after a period of neoadjuvant chemo-radiation therapy. Magnetic resonance imaging/magnetic resonance cholangiopancreatography, positron emission tomography scan, endoscopic ultrasound and computed tomography scans are the most frequently used modalities for diagnosis and tumor staging. Adjuvant therapy, palliative chemotherapy and radiotherapy have been relatively ineffective for inoperable CC. For most of these patients biliary stenting provides effective palliation. Photodynamic therapy is an emerging palliative treatment that seems to provide pain relief, improve biliary patency and increase survival. The clinical utility of other emerging therapies such as transarterial chemoembolization, hepatic arterial chemoinfusion and high intensity intraductal ultrasound needs further study.
Figures
References
-
- Olnes MJ, Erlich R. A review and update on cholangiocarcinoma. Oncology. 2004;66:167–179. - PubMed
-
- Shaib Y, El-Serag HB. The epidemiology of cholangiocarcinoma. Semin Liver Dis. 2004;24:115–125. - PubMed
-
- Watanapa P. Cholangiocarcinoma in patients with opisthorchiasis. Br J Surg. 1996;83:1062–1064. - PubMed
-
- Cook DJ, Mulrow CD, Haynes RB. Systematic reviews: synthesis of best evidence for clinical decisions. Ann Intern Med. 1997;126:376–380. - PubMed
-
- Mulrow CD, Oxman AD. Cochrane Collaboration Handbook. Vol. 126. Oxford: Update Software; 1997. p. 1.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
