

Meta-analysis and systematic review of colorectal endoscopic mucosal resection
- PMID: 19750569
- PMCID: PMC2744182
- DOI: 10.3748/wjg.15.4273
Meta-analysis and systematic review of colorectal endoscopic mucosal resection
Abstract
Aim: To evaluate the proportion of successful complete cure en-bloc resections of large colorectal polyps achieved by endoscopic mucosal resection (EMR).
Methods: Studies using the EMR technique to resect large colorectal polyps were selected. Successful complete cure en-bloc resection was defined as one piece margin-free polyp resection. Articles were searched for in Medline, Pubmed, and the Cochrane Control Trial Registry, among other sources.
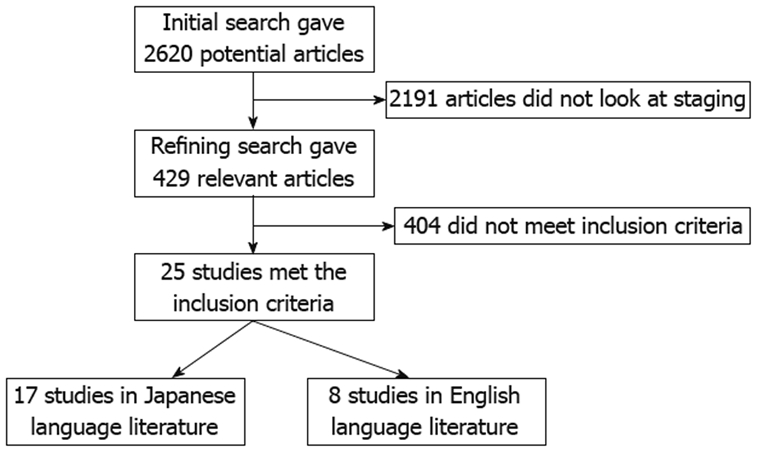
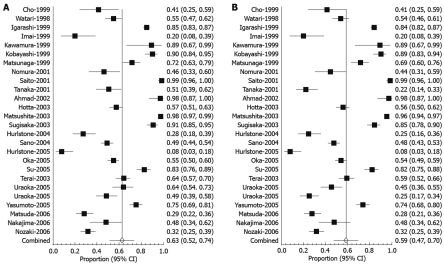
Results: An initial search identified 2620 reference articles, from which 429 relevant articles were selected and reviewed. Data was extracted from 25 studies (n = 5221) which met the inclusion criteria. All the studies used snares to perform EMR. Pooled proportion of en-bloc resections using a random effect model was 62.85% (95% CI: 51.50-73.52). The pooled proportion for complete cure en-bloc resections using a random effect model was 58.66% (95% CI: 47.14-69.71). With higher patient load (> 200 patients), this complete cure en-bloc resection rate improves from 44.19% (95% CI: 24.31-65.09) to 69.17% (95% CI: 51.11-84.61).
Conclusion: EMR is an effective technique for the resection of large colorectal polyps and offers an alternative to surgery.
Figures
References
-
- Kojima T, Parra-Blanco A, Takahashi H, Fujita R. Outcome of endoscopic mucosal resection for early gastric cancer: review of the Japanese literature. Gastrointest Endosc. 1998;48:550–554; discussion 554-555. - PubMed
-
- Gotoda T, Kondo H, Ono H, Saito Y, Yamaguchi H, Saito D, Yokota T. A new endoscopic mucosal resection procedure using an insulation-tipped electrosurgical knife for rectal flat lesions: report of two cases. Gastrointest Endosc. 1999;50:560–563. - PubMed
-
- Conio M, Cameron AJ, Chak A, Blanchi S, Filiberti R. Endoscopic treatment of high-grade dysplasia and early cancer in Barrett's oesophagus. Lancet Oncol. 2005;6:311–321. - PubMed
-
- Fukami N, Lee JH. Endoscopic treatment of large sessile and flat colorectal lesions. Curr Opin Gastroenterol. 2006;22:54–59. - PubMed
-
- Zlatanic J, Waye JD, Kim PS, Baiocco PJ, Gleim GW. Large sessile colonic adenomas: use of argon plasma coagulator to supplement piecemeal snare polypectomy. Gastrointest Endosc. 1999;49:731–735. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
