

Practice parameter: Evaluation of the child with microcephaly (an evidence-based review) [RETIRED]: report of the Quality Standards Subcommittee of the American Academy of Neurology and the Practice Committee of the Child Neurology Society
- PMID: 19752457
- PMCID: PMC2744281
- DOI: 10.1212/WNL.0b013e3181b783f7
Practice parameter: Evaluation of the child with microcephaly (an evidence-based review) [RETIRED]: report of the Quality Standards Subcommittee of the American Academy of Neurology and the Practice Committee of the Child Neurology Society
Abstract
Objective: To make evidence-based recommendations concerning the evaluation of the child with microcephaly.
Methods: Relevant literature was reviewed, abstracted, and classified. RECOMMENDATIONS were based on a 4-tiered scheme of evidence classification.
Results: Microcephaly is an important neurologic sign but there is nonuniformity in its definition and evaluation. Microcephaly may result from any insult that disturbs early brain growth and can be seen in association with hundreds of genetic syndromes. Annually, approximately 25,000 infants in the United States will be diagnosed with microcephaly (head circumference <-2 SD). Few data are available to inform evidence-based recommendations regarding diagnostic testing. The yield of neuroimaging ranges from 43% to 80%. Genetic etiologies have been reported in 15.5% to 53.3%. The prevalence of metabolic disorders is unknown but is estimated to be 1%. Children with severe microcephaly (head circumference <-3 SD) are more likely ( approximately 80%) to have imaging abnormalities and more severe developmental impairments than those with milder microcephaly (-2 to -3 SD; approximately 40%). Coexistent conditions include epilepsy ( approximately 40%), cerebral palsy ( approximately 20%), mental retardation ( approximately 50%), and ophthalmologic disorders ( approximately 20% to approximately 50%).
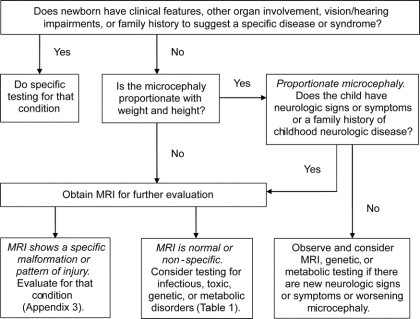
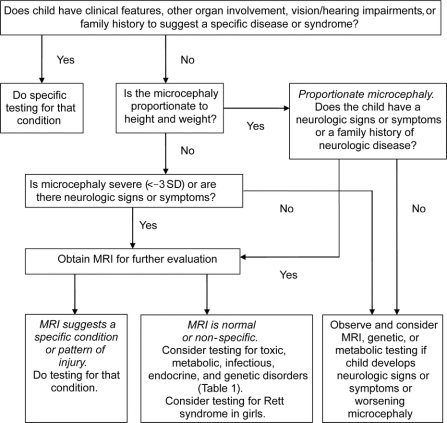
Recommendations: Neuroimaging may be considered useful in identifying structural causes in the evaluation of the child with microcephaly (Level C). Targeted and specific genetic testing may be considered in the evaluation of the child with microcephaly who has clinical or imaging abnormalities that suggest a specific diagnosis or who shows no evidence of an acquired or environmental etiology (Level C). Screening for coexistent conditions such as cerebral palsy, epilepsy, and sensory deficits may also be considered (Level C). Further study is needed regarding the yield of diagnostic testing in children with microcephaly.
Figures
Comment in
-
Practice parameter: evaluation of the child with microcephaly (an evidence-based review): report of the quality standards subcommittee of the American Academy Of Neurology and the Practice Committee Of The Child Neurology Society.Neurology. 2010 Mar 30;74(13):1079-80; author reply 1080. doi: 10.1212/WNL.0b013e3181d5e057. Neurology. 2010. PMID: 20350982 No abstract available.
-
Practice parameter: evaluation of the child with microcephaly (an evidence-based review): report of the quality standards subcommittee of the American Academy of Neurology and the Practice Committee of the Child Neurology Society.Neurology. 2010 Mar 30;74(13):1079; author reply 1079. doi: 10.1212/WNL.0b013e3181d5dfca. Neurology. 2010. PMID: 20350983 No abstract available.
-
Practice parameter: evaluation of the child with microcephaly (an evidence-based review): report of the quality standards subcommittee of the American Academy of Neurology and the Practice Committee of the Child Neurology Society.Neurology. 2010 Mar 30;74(13):1080-1; author reply 1081. doi: 10.1212/WNL.0b013e3181d5e077. Neurology. 2010. PMID: 20350984 No abstract available.
References
-
- Leviton A, Holmes LB, Allred EN, Vargas J. Methodologic issues in epidemiologic studies of congenital microcephaly. Early Hum Dev 2002;69:91–105. - PubMed
-
- Opitz JM, Holt MC. Microcephaly: general considerations and aids to nosology. J Craniofac Genet Dev Biol 1990;10:75–204. - PubMed
-
- Roche AF, Mukherjee D, Guo SM, Moore WM. Head circumference reference data: birth to 18 years. Pediatrics 1987;79:706–712. - PubMed
-
- Barkovich AJ, Ferriero DM, Barr RM, et al. Microlissencephaly: a heterogeneous malformation of cortical development. Neuropediatrics 1999;29:113–119. - PubMed
-
- Dobyns WB, Andermann E, Andermann F, et al. X-linked malformations of neuronal migration. Neurology 1996;47:331–339. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources