

Motivational intervention to reduce rapid subsequent births to adolescent mothers: a community-based randomized trial
- PMID: 19752472
- PMCID: PMC2746510
- DOI: 10.1370/afm.1014
Motivational intervention to reduce rapid subsequent births to adolescent mothers: a community-based randomized trial
Abstract
Purpose: One-quarter of adolescent mothers bear another child within 2 years, compounding their risk of poorer medical, educational, economic, and parenting outcomes. Most efforts to prevent rapid subsequent birth to teenagers have been unsuccessful but have seldom addressed motivational processes.
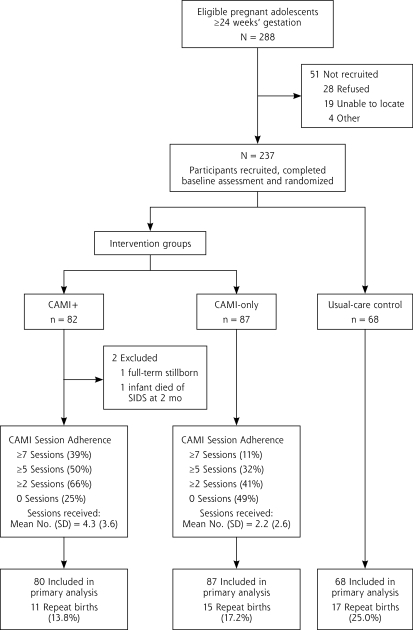
Methods: We conducted a randomized trial to determine the effectiveness of a computer-assisted motivational intervention (CAMI) in preventing rapid subsequent birth to adolescent mothers. Pregnant teenagers (N = 235), aged 18 years and older who were at more than 24 weeks' gestation, were recruited from urban prenatal clinics serving low-income, predominantly African American communities. After completing baseline assessments, they were randomly assigned to 3 groups: (1) those in CAMI plus enhanced home visit (n = 80) received a multi-component home-based intervention (CAMI+); (2) those in CAMI-only (n = 87) received a single component home-based intervention; (3) and those in usual-care control (n = 68) received standard usual care. Teens in both intervention groups received CAMI sessions at quarterly intervals until 2 years' postpartum. Those in the CAMI+ group also received monthly home visits with parenting education and support. CAMI algorithms, based on the transtheoretical model, assessed sexual relationships and contraception-use intentions and behaviors, and readiness to engage in pregnancy prevention. Trained interventionists used CAMI risk summaries to guide motivational interviewing. Repeat birth by 24 months' postpartum was measured with birth certificates.
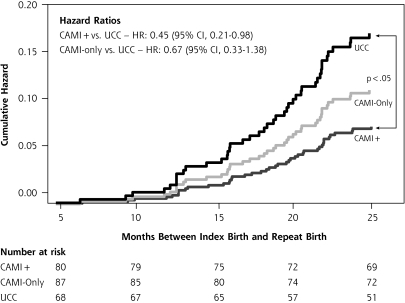
Results: Intent-to-treat analysis indicated that the CAMI+ group compared with the usual-care control group exhibited a trend toward lower birth rates (13.8% vs 25.0%; P = .08), whereas the CAMI-only group did not (17.2% vs 25.0%; P = .32). Controlling for baseline group differences, the hazard ratio (HR) for repeat birth was significantly lower for the CAMI+ group than it was with the usual-care group (HR = 0.45; 95% CI, 0.21-0.98). We developed complier average causal effects models to produce unbiased estimates of intervention effects accounting for variable participation. Completing 2 or more CAMI sessions significantly reduced the risk of repeat birth in both groups: CAMI+ (HR = 0.40; 95% CI, 0.16-0.98) and CAMI-only (HR = 0.19; 95% CI, 0.05-0.69).
Conclusions: Receipt of 2 or more CAMI sessions, either alone or within a multicomponent home-based intervention, reduced the risk of rapid subsequent birth to adolescent mothers.
Figures
References
-
- Schelar E, Franzetta K, Manlove J. Repeat teen childbearing: differences across states and by race and ethnicity. Washington DC: Child Trends Research Brief. http://www.childtrends.org/Files//Child_Trends-2007_11_27_RB_RepeatCB.pdf Accessed May 12, 2008.
-
- Klerman LV. Another Chance: Preventing Additional Births to Teen Mothers. Washington DC: National Campaign to Prevent Teen Pregnancy; 2004.
-
- US Department of Health and Human Services. Healthy People 2010: Understanding and Improving Health. 2nd ed. Washington, DC: US Government Printing Office; 2000.
-
- Furstenberg FF Jr, Levine JA, Brooks-Gunn J. The children of teenage mothers: patterns of early childbearing in two generations. Fam Plann Perspect. 1990;22(2):54–61. - PubMed
-
- Pogarsky G, Thornberry TP, Lizotte AJ. Developmental outcomes for children of young mothers. J Marriage Fam. 2006;68(2):332–344.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical