

Venous retinal flow reperfusion mechanisms following radial optic neurotomy with adjunctive intraocular triamcinolone in central retinal vein occlusion
- PMID: 19756692
- PMCID: PMC2801847
- DOI: 10.1007/s00417-009-1187-2
Venous retinal flow reperfusion mechanisms following radial optic neurotomy with adjunctive intraocular triamcinolone in central retinal vein occlusion
Abstract
Background: To evaluate retinal reperfusion, anastomosis, and compensation following radial optic neurotomy for ischemic nonperfused central retinal vein occlusion.
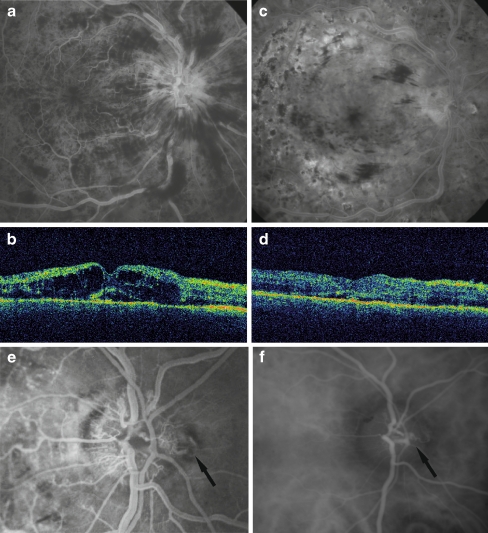
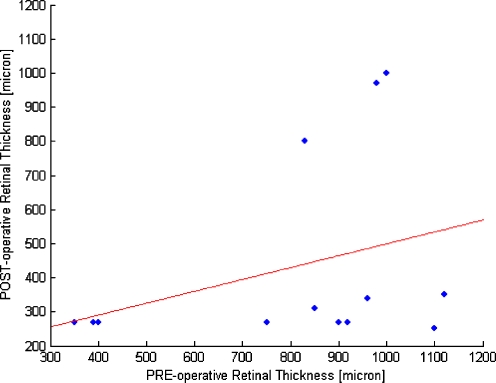
Methods: Prospective, non-comparative, interventional case series of 13 patients with ischemic, nonperfused central retinal vein occlusion who underwent decompression surgery with a radial optic neurotomy and adjunctive intraocular triamcinolone. Patients were followed for 1 year after surgery, and were analyzed in the preoperative and postoperative stages determining: visual acuity by ETDRS chart (LogMar) and retinal thickness with optical coherence tomography. Fluorescein angiography was performed at regular intervals to evaluate the capillary perfusion grade. Intraocular pressure was measured and fundus was examined.
Results: Visual acuity and retinal thickness improved in 10/13 (77%) patients after surgery at 1-year follow-up. Adequate retinal reperfusion was achieved in ten of the 13 eyes. Acute reperfusion occurred in six eyes within 2 weeks of surgery and a shunt vessel at the optic disk developed in four eyes within 4 months. In the remaining three eyes, retinal reperfusion was not observed by fluorescein angiography. No complications were noted in any of the patients.
Conclusion: Surgical decompression promoted mechanical reperfusion of the occluded vessel in 10/13 (77%) cases. In 6/13 patients (46%) reperfusion occurred within 2 weeks of surgery, and in 4/13 patients (31%) collateral vessels formed within 4 months.
Figures



References
-
- The Eye Disease Case-Control Study Group Risk factors for central retinal vein occlusion. Arch Ophthalmol. 1996;114:545–554. - PubMed
-
- Rath EZ, Frank RN, Shin DH, Kim C. Risk factors for retinal vein occlusions: a case-controlled study. Ophthalmology. 1992;99:509–514. - PubMed
-
- Hayreh SS. Retinal vein occlusion. Indian J Ophthalmol. 1994;42:109–132. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
