

Endoscopic and percutaneous preoperative biliary drainage in patients with suspected hilar cholangiocarcinoma
- PMID: 19756881
- PMCID: PMC2793391
- DOI: 10.1007/s11605-009-1009-1
Endoscopic and percutaneous preoperative biliary drainage in patients with suspected hilar cholangiocarcinoma
Abstract
Introduction: Controversy exists over the preferred technique of preoperative biliary drainage (PBD) in patients with hilar cholangiocarcinoma (HCCA) requiring major liver resection. The current study compared outcomes of endoscopic biliary drainage (EBD) and percutaneous transhepatic biliary drainage (PTBD) in patients with resectable HCCA.
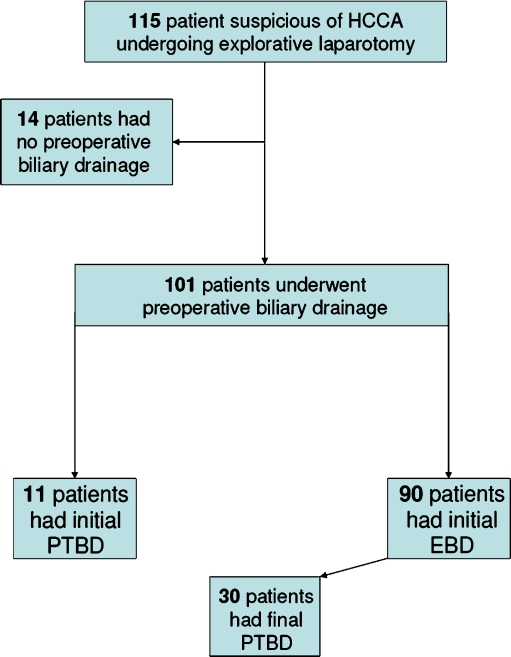
Methods: One hundred fifteen consecutive patients were explored for HCCA between 2001 and July 2008 and assigned by initial PBD procedure to either EBD or PTBD.
Results: Of these patients, 101 (88%) underwent PBD; 90 patients underwent EBD as primary procedure, and 11 PTBD. The technical success rate of initial drainage was 81% in the EBD versus 100% in the PTBD group (P = 0.20). Stent dislocation was similar in the EBD and PTBD groups (23% vs. 20%, P = 0.70). Infectious complications were significantly more common in the endoscopic group (48% vs. 9%, P < 0.05). Patients in the EBD group underwent more drainage procedures (2.8 vs. 1.4, P < 0.01) and had a significantly longer drainage period until laparotomy (mean 15 weeks vs. 11 weeks in the PTBD group; P < 0.05). In 30 patients, EBD was converted to PTBD due to failure of the endoscopic approach.
Conclusions: Preoperative percutaneous drainage could outperform endoscopic stent placement in patients with resectable HCCA, showing fewer infectious complications, using less procedures.
Figures
References
-
- Saiki S, Chijiiwa K, Komura M, Yamaguchi K, Kuroki S, Tanaka M. Preoperative internal biliary drainage is superior to external biliary drainage in liver regeneration and function after hepatectomy in obstructive jaundiced rats. Ann Surg. 1999;230:655–662. doi: 10.1097/00000658-199911000-00007. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
